
Guide to Coding Software Terminology
Mastering medical coding software terminology is no longer optional—it’s essential for accurate billing, faster reimbursements, and audit-proof documentation. Whether you’re handling inpatient DRG coding or outpatient E/M levels, fluency in system terms like claim batches, NPI crosswalks, clearinghouse rejections, and encounter-level edits means you can code, troubleshoot, and bill with confidence. The learning curve isn’t just clinical—it’s technical.
Every EHR and coding platform—Epic, Cerner, eClinicalWorks, or AdvancedMD—uses its own workflows, but the terminology stays foundational across systems. Understanding coding software vocabulary bridges the gap between what providers document and what payers approve. This guide will take you deep into platform-agnostic coding terms, system-specific nuances, and real-world terminology taught inside AMBCI’s Coding & Software Certification, making sure you’re job-ready for any billing platform, specialty, or payer rule set.

Common Programming Concepts Across All Platforms
Code Sets, Modifiers, Encounters, Claim Batches
Every medical coding system—whether it's Epic, Kareo, AdvancedMD, or eClinicalWorks—relies on the same foundational structure: code sets, modifiers, encounters, and claim batches. These aren't just data points—they dictate how services are reported, billed, and reimbursed.
ICD-10-CM codes document diagnoses.
CPT/HCPCS codes represent procedures or services.
Modifiers like -25, -59, and -76 alter meanings to reflect visit complexity or duplication avoidance.
An encounter reflects a visit tied to patient ID, provider, payer, and date of service.
Claim batches bundle multiple encounters into a single submission file for payers or clearinghouses.
Whether you’re coding a level 4 E/M for urgent care or tagging a bilateral surgical procedure, knowing how these components interlock is critical for clean claims and reduced rework.
Edits, Rejections, Payer Rules
Once codes are entered, software logic determines if a claim is ready to go—or destined for denial. Edits, rejections, and payer-specific rules are the filters every claim must pass through.
Edits are automated checks that flag errors like invalid diagnosis-procedure pairing, missing NPI, or duplicate charges.
Rejections occur at the clearinghouse level, preventing transmission to payers due to formatting or data validation issues.
Denials happen after payer review, and may cite non-covered services, lack of medical necessity, or authorization errors.
Each platform handles this differently. In Optum EncoderPro, you'll see payer-specific edits. In 3M or TruCode, you'll navigate grouped edits for compliance and sequencing. Coders must quickly identify the source—was it a software flag, clearinghouse rejection, or payer denial?—to correct claims efficiently.
Audit Trails, Coding Compliance, Productivity Metrics
Beyond correct coding, medical software tracks what was coded, how fast, and whether it's compliant. Terms like audit trail, compliance edit, and coder productivity show up in almost every interface—but few understand how to use them strategically.
Audit trail logs show when a user modifies a claim or note, essential for both internal audits and external payer inquiries.
Compliance edits enforce rules from CMS, AMA, or payer contracts, such as flagging unbundled procedures or misused modifiers.
Coder productivity is tracked using metrics like charts coded per hour, first-pass clean claim rate, and denial overturn ratio.
Understanding where to find and interpret these in tools like AthenaCollector, DrChrono, or NextGen gives coders an edge. It’s not just about speed—it’s about accuracy that holds up under payer scrutiny and CMS audit protocols. The top 5% of coders understand software language as fluently as they understand anatomy and guidelines.

Language-Specific Terminology Explained
Epic: SmartTools, Chart Review, Encounter-Level Edits
Epic Systems has one of the most complex terminologies in medical software, especially when navigating the coding layer within clinical workflows.
SmartTools include SmartPhrases and SmartTexts—predefined text modules coders use to streamline documentation and improve billing accuracy. These can be auto-linked to coding suggestions or templates.
Chart Review provides access to previous encounters, lab results, and prior procedures. It is essential for ensuring diagnosis linkage continuity.
Encounter-level edits are triggered before claims leave the system—flagging coding inconsistencies like missing linking diagnoses or unsupported modifier use.
Coders using Epic must understand how coding workflows are embedded within clinical templates, affecting both speed and compliance risk.
Cerner: PowerChart, Discern Analytics, Charge Capture
Cerner’s medical coding language is built around real-time interaction between clinical notes and coding logic.
PowerChart is Cerner’s interface for documentation and coding. Within it, coders access encounter details, linked CPTs, and modifiers.
Discern Analytics pulls coding performance data, highlighting trends like frequent denials, code usage variance, and provider documentation gaps.
Charge capture tools integrate with provider workflows, allowing coders to validate services before charges are sent.
Cerner coders must master cross-module terminology, especially as charge rules differ across specialties and payer profiles.
AdvancedMD: Charge Slips, Code Pick Lists, Claim Inspector
AdvancedMD streamlines coding workflows, but its terminology introduces a different ecosystem altogether.
Charge Slips are digital equivalents of superbills—coders must match services performed to CPT codes using predefined templates.
Code Pick Lists are customized CPT/ICD-10 lists tailored by specialty or provider preference—misusing them can lead to undercoding or denials.
Claim Inspector is a pre-submission tool that checks claims against payer rules and compliance guidelines—similar to front-end edits.
Coders using AdvancedMD must know how to manage claim staging, interpret rejection alerts, and adjust pick lists based on denial patterns.
| Feature | Epic | Cerner | AdvancedMD |
|---|---|---|---|
| Documentation Tools | SmartTools (SmartPhrases, SmartTexts) | PowerChart – clinical note + coding interface | Charge Slips – digital superbills |
| Historical Data Access | Chart Review – previous encounters, labs, procedures | Embedded in PowerChart | N/A |
| Coding Alerts | Encounter-Level Edits – real-time flags | Charge Capture – validates charges in workflow | Claim Inspector – pre-submission claim check |
| Analytics & Feedback | N/A | Discern Analytics – denial trends, documentation gaps | Claim Inspector denial patterns and rejection tracking |
| Customization Tools | Template-linked SmartTexts | Specialty-specific charge rules | Code Pick Lists – customizable CPT/ICD lists |
| Compliance Layer | Integrated within clinical templates | Varies by specialty module | Claim Inspector enforces payer-specific rules |
Version Control Systems Explained
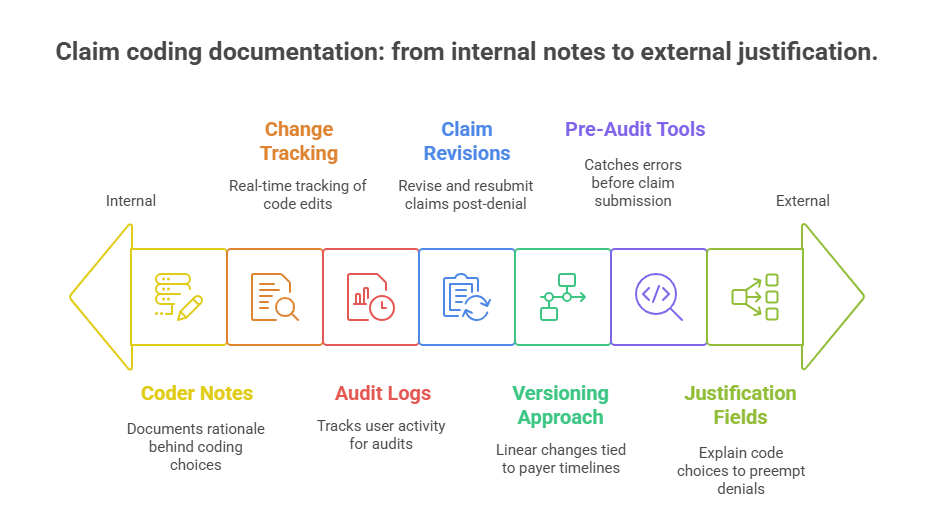
Claim Revisions, Audit Logs, Change Tracking
While medical coding doesn’t use Git or GitHub, it relies on an equivalent form of version control—through claim revisions, audit logs, and change tracking inside EHR and billing platforms.
Claim revisions occur when a previously submitted claim is modified, often after a denial, payer policy update, or provider documentation change. Systems like eClinicalWorks and Kareo allow coders to clone and resubmit adjusted claims with full history retained.
Audit logs track every change: who entered a diagnosis, when a modifier was removed, or how a denial was resolved. These logs are essential during Medicare audits or payer record requests.
Change tracking flags edits in real time. For instance, Epic’s Claim Edit History or AdvancedMD’s Activity Log visually show which codes were added, replaced, or rejected across versions.
Coders fluent in revision terminology can isolate issues faster, submit corrected claims cleanly, and withstand retrospective audits without delay.
Notes, Justification Fields, Pre-Audit Tools
Modern coding systems include built-in controls to justify every coding decision, mimicking the commit messages used in software dev.
Coder notes—often called “internal remarks” or “sticky notes”—explain why a code or modifier was used.
Justification fields prompt for supporting language or chart excerpts to validate medical necessity before claim submission.
Pre-audit tools, like Claim Scrubbers, simulate payer edits to catch inconsistencies. Tools like ZirMed, Optum One, and TruCode Analyzer automate this process.
Unlike Git branches, medical coding doesn’t fork workflows—it iterates claims, tied to payer timelines and provider documentation. A coder's ability to track these iterations without data loss or documentation gaps determines both cash flow and audit defensibility.
Web Development Software Terminology
Front-End: Dashboards, API Feeds, Real-Time Alerts
In web-based medical coding systems, the front-end interface isn’t just visual—it’s where coders interact with live claim data, alerts, and payer integrations.
Dashboards display key performance indicators (KPIs): clean claim rate, denial trends, average AR days, and rejection frequency. Coders rely on these to spot patterns and prioritize corrections.
API feeds allow real-time syncing between EHRs and third-party tools like clearinghouses (Availity, Office Ally) or coding platforms (TruCode, 3M). These feeds auto-populate codes, insurance info, and even payment statuses into the coder’s view.
Real-time alerts warn of invalid code combinations or missing authorizations before claim submission—saving hours in rework.
Coders using cloud-based tools like DrChrono, Kareo, or Athenahealth must understand front-end logic, not just clinical notes. Each click triggers a backend action—and small missteps can create massive billing errors.
Back-End: Data Mapping, Middleware, Eligibility Checks
Behind the scenes, back-end systems handle complex logic—mapping patient data to code sets, validating insurance, and routing claims.
Data mapping refers to how patient information, diagnoses, and procedures are translated into billing data formats, like ANSI X12 for electronic claims (837P, 835).
Middleware bridges different systems—EHRs, clearinghouses, payers—so coders can see seamless transitions even across vendors.
Eligibility checks confirm payer coverage before coding even begins. These are usually automated but may need manual overrides if API feeds fail or payer databases return ambiguous results.
Understanding these terms lets coders anticipate system behavior—why a claim gets held, where data drops off, and how to correct issues without resubmitting entire batches.
Full-Stack Integration: EHRs, RCMs, Clearinghouses
A truly integrated coding environment involves EHR software, revenue cycle management (RCM) tools, and clearinghouses working together.
EHRs house the clinical notes coders work from. Examples: Epic, Cerner, NextGen.
RCM systems handle the financial logic—tracking charges, remits, denials, and payments. Examples: AthenaCollector, Azalea Health, CareCloud.
Clearinghouses serve as traffic controllers—formatting and forwarding claims, returning rejections, and logging payer responses.
Coders fluent in full-stack terminology can operate across this triad—pushing clean claims, interpreting responses, and navigating complex payer requirements with minimal supervision.
| Feature | Front-End | Back-End | Full-Stack Integration |
|---|---|---|---|
| Core Purpose | User interface for interacting with claims and real-time data | Handles data processing, validation, and system communication | Seamless coordination between clinical, financial, and transmission systems |
| Key Tools/Concepts | Dashboards, API Feeds, Real-Time Alerts | Data Mapping, Middleware, Eligibility Checks | EHRs, RCM Platforms, Clearinghouses |
| Example Functions | Shows KPIs, triggers alerts for missing codes or auth, updates from APIs | Translates clinical data into 837P/835, validates insurance, bridges multiple systems | Enables coders to push, monitor, and troubleshoot claims across entire pipeline |
| Software Examples | DrChrono, Kareo, Athenahealth | Integrated services within backend of Epic, Cerner, AdvancedMD | Epic (EHR), AthenaCollector (RCM), Availity/Office Ally (Clearinghouse) |
| Coder Responsibilities | Interpret alerts, monitor KPIs, correct claims before submission | Understand system logic, fix data mismatches, handle API or middleware errors | Navigate across tools, resolve rejection causes, and ensure clean claim flow |
Popular IDEs and Their Jargon
Interfaces: Code Search, Charge Capture, Coding Panels
Medical coders don’t use IDEs like developers—but coding platforms have their own powerful interfaces, often with deep customization and shortcuts tailored for speed and accuracy.
Code search tools within systems like TruCode, 3M Encoder, or Find-A-Code allow rapid lookup by keyword, code, or clinical condition. Some include automated suggestions based on linked documentation or problem lists.
Charge capture modules let providers select services performed, which coders then verify, modify, or append with supporting codes (e.g., adding modifiers, validating POS codes).
Coding panels are dedicated windows—often side-by-side with progress notes or encounter summaries—where ICD-10, CPT, and HCPCS codes are entered, verified, or edited.
Knowing how to navigate these panels efficiently improves turnaround time and reduces first-pass rejections.
Common Functions: Linter, Template Builder, Reimbursement Estimators
Medical coding platforms include embedded logic checkers and automation tools that mirror developer IDE features.
Linter equivalents in coding tools are real-time edit validators—flagging unlinked diagnoses, outdated codes, or NCCI violations.
Template builders let practices preconfigure coding sheets by specialty, visit type, or provider—ensuring coders don’t start from scratch for each encounter.
Reimbursement estimators, often payer-integrated, give coders real-time insight into expected payment amounts based on selected codes and contracts.
Tools like Athenahealth’s coding rules engine or eClinicalWorks’ Superbill Designer reduce cognitive load. Coders using these features consistently hit productivity and accuracy benchmarks above industry averages.

Software Development Lifecycle (SDLC) Terms
Agile, Scrum, Sprint, Kanban in Medical Coding
Coding departments in larger health systems are adopting Agile-inspired workflows—mirroring software teams for faster claim turnarounds and cleaner submissions.
Agile in medical coding focuses on iterative claim review cycles, where batches are scrubbed, adjusted, and finalized in loops based on payer feedback or policy updates.
A Scrum team may include coders, billers, auditors, and a project manager overseeing turnaround KPIs.
A sprint might last 1–2 weeks, aimed at clearing backlogged claims or adjusting CPTs after guideline changes (e.g., the 2025 E/M updates).
Kanban boards, built into tools like Jira, Athenahealth Task Flow, or even Trello, visualize where each claim or chart stands—uncoded, pending review, edited, sent.
Agile terms in coding aren’t just buzzwords—they reflect real operational processes that reduce denials and increase cash flow velocity.
Waterfall, DevOps, MVP, Release Cycles
While Agile dominates outpatient settings, Waterfall models still appear in hospital inpatient coding or long-term care RCM systems.
Waterfall here means sequential: documentation, abstraction, coding, review, submission. It’s rigid but reliable when volume is high and variation is low.
DevOps parallels emerge in integrated EHR/RCM environments—where coders, IT, and compliance teams coordinate claim templates, payer rules, and scrubber logic updates.
MVP (Minimum Viable Product) in coding translates to getting claims out with just enough data to avoid rejection, before adding complex modifiers or linked services.
Release cycles happen when payer edits, NCCI updates, or CPT code changes roll out—coders must adapt templates, workflows, and training accordingly.
Each coding system—Epic, Cerner, Azalea Health, DrChrono—manages updates differently. Some push silent patches; others require coders to manually reconfigure mappings or templates. The best coders track these cycles proactively and adjust workflows before claim failures spike.
Whether you're in a two-person practice or coding for a 1,000-bed health system, knowing the cycle your team follows—and the terms used to optimize it—makes you faster, more accurate, and more promotable.
| SDLC Term | Medical Coding Adaptation | Function & Use Case |
|---|---|---|
| Agile | Iterative claim reviews, adjusting based on payer feedback or policy changes | Promotes fast turnaround, clean claims, and adaptability in dynamic environments |
| Scrum | Teams include coders, billers, auditors, and a PM managing KPIs and workflows | Improves collaboration and structured progress toward coding and billing goals |
| Sprint | Short-term coding cycles (1–2 weeks) to clear backlogs or apply new guidelines | Focuses efforts on timely, goal-driven claim completion and update implementation |
| Kanban | Visual task tracking (e.g., uncoded, pending review, sent) via Trello or Athenahealth | Provides real-time workflow visibility and reduces missed or delayed submissions |
| Waterfall | Sequential process: documentation → coding → review → submission | Best for inpatient settings or high-volume, predictable workflows |
| DevOps | Collaboration between coders, IT, and compliance to update logic and scrubbers | Improves coordination and prevents system lag during payer or regulation updates |
| MVP (Minimum Viable Product) | Submitting basic valid claims first, appending complex codes or documentation later | Ensures timely submission while allowing follow-up adjustments when needed |
| Release Cycles | Template and workflow updates tied to CPT/NCCI/payer revisions | Coders must proactively adapt to maintain compliance and avoid rejections |
How AMBCI’s Medical Billing and Coding Certification Equips You With Practical Coding Knowledge
Real-World Tools, Not Just Theory
The AMBCI Medical Billing and Coding Certification goes beyond textbook ICD-10 or CPT memorization—it trains you in the exact software tools used by hospitals, clinics, and billing companies. From navigating claim scrubbers in TruCode to simulating denial workflows in AthenaCollector, every module is built to mirror how real coding platforms function.
You won’t just learn what a modifier is—you’ll see how software flags modifier misuse, how to correct it, and how it impacts reimbursement. Through live-case coding, productivity simulations, and scenario-based drills, the program builds confident, audit-ready coders trained to deliver clean claims on the first pass.
Taught Terminology for Hiring-Readiness
Hiring managers don’t just want coding accuracy—they want coders who speak the language of billing platforms. That means knowing the difference between a front-end scrubber edit and a payer-side denial, how to escalate an issue in an RCM dashboard, or when to use templates vs. custom CPT entries.
This certification embeds that terminology into every lesson—terms like rejection loop, encounter-level validation, and claim bundling logic aren’t afterthoughts—they’re built-in from Day 1. You graduate speaking the same operational language as the systems you’ll be working on.
Applicable Across EHRs, Web Platforms, and Clearinghouses
Whether your employer uses Epic, Kareo, DrChrono, or NextGen, this certification ensures you're fluent across platforms. AMBCI’s course includes crosswalk training—teaching how to adapt coding workflows across systems with different layouts, data fields, and claim logic.
By learning how clearinghouses like Availity handle batches, how eClinicalWorks populates code suggestions, or how 3M handles CCI edits, you'll move between platforms without retraining—making you a more flexible, more valuable hire.
Frequently Asked Questions
-
To get hired in today’s medical coding roles, you must know how to use coding platforms like 3M Encoder, TruCode, and Optum EncoderPro. Most jobs also expect fluency in EHR systems like Epic, Cerner, or eClinicalWorks, as well as clearinghouse portals such as Availity or Office Ally. You’ll also need to understand claim scrubbing software, denial management dashboards, and code lookup systems that support ICD-10-CM, CPT, and HCPCS coding. The AMBCI Medical Billing and Coding Certification trains students to use these tools in real-world workflows, so they can transition directly into high-performance coding teams without additional on-the-job training.
-
While AAPC and AHIMA focus heavily on theoretical coding knowledge and national exams, AMBCI’s Medical Billing and Coding Certification blends that with intensive platform training. Students learn ICD-10-CM, CPT, and HCPCS just like AAPC’s CPC or AHIMA’s CCS programs—but they also get real exposure to claim cycle software, denial resolution tools, and RCM dashboards. This makes AMBCI graduates more job-ready and versatile across different EHRs and billing systems. It’s ideal for coders looking to enter the workforce faster with hands-on knowledge of how actual claim workflows operate in real practices and hospitals.
-
A rejection means the claim didn’t make it past the clearinghouse due to formatting errors or missing data—no payer ever reviewed it. A denial, on the other hand, means the payer reviewed and refused to pay based on policy violations, lack of documentation, or incorrect coding logic. Rejections require quick software corrections; denials may need appeals, chart reviews, or modifier adjustments. The AMBCI program teaches students how to interpret rejection messages from clearinghouses like Availity, and how to resolve payer denials using claim audit tools and compliance logic embedded in coding platforms.
-
AMBCI covers all three major code sets: ICD-10-CM (diagnosis coding), CPT (procedural coding), and HCPCS Level II (medical supplies, durable equipment, ambulance services, and drugs). Students also learn how these codes interact with modifiers, payer rules, and NCCI edits. Beyond theory, the certification teaches how software applies these codes in claim generation, encounter documentation, and payer logic engines. Unlike static textbook courses, AMBCI uses platform simulations and software walkthroughs to train coders in how and when to use each code set correctly—especially within specialty-specific workflows like cardiology, dermatology, and surgery.
-
Yes. Remote medical coding roles are increasing across hospitals, private practices, and outsourcing agencies. Employers look for coders who are independent, compliant, and platform-proficient. AMBCI’s certification prepares graduates for remote work by emphasizing digital workflow fluency, including how to log in to cloud-based EHRs, use screen-sharing tools for audit review, and manage coding queues using remote RCM dashboards. You’ll also be trained to handle HIPAA-compliant documentation practices, so you can safely and legally code from home without risking PHI exposure or audit violations.
-
Most students complete the AMBCI Medical Billing and Coding Certification in 7 to 12 weeks, depending on their pace. It’s a self-paced online program with access to 200+ modules, simulations, assessments, and coding exercises. You can move faster if you have prior healthcare or EHR experience—or take your time to fully master the material. Each lesson includes interactive coding software tutorials, real-case claim walkthroughs, and exam-prep style quizzes to ensure retention. Students can revisit lessons anytime, and access does not expire—making it one of the most flexible and job-ready programs available online.
-
Payers like Medicare, Medicaid, Blue Cross, and Aetna all have slightly different rules for code acceptance, modifier use, and documentation standards. AMBCI’s certification trains you to recognize and work within these variations using platform-based payer logic tools. For example, you’ll learn how to configure claim templates for Medicare NCCI edits, use payer response codes to resolve denials, and adjust logic based on local coverage determinations (LCDs). Rather than memorizing every rule, you’ll learn how software interprets and applies payer policies—a far more scalable skillset in high-volume billing environments.
Summing Up: Speak Software Fluently
Mastering medical coding software terminology is the fastest way to rise above entry-level. It’s not enough to know CPT or ICD-10—you must understand how platforms interpret those codes, how rejections are triggered, and how real-time edits affect cash flow. Whether you're using 3M, Epic, or Kareo, fluency in system language makes you not just a coder—but a problem-solver, auditor, and revenue defender.
The AMBCI Medical Billing and Coding Certification gives you that edge. You’ll graduate speaking the language of billing software, clearinghouses, and payer logic—ready to code with speed, accuracy, and confidence. In a job market where productivity and compliance rule, this isn’t a bonus. It’s essential.
If you're ready to turn coding knowledge into job-ready skills, this is your moment to move forward—faster, smarter, and fully equipped.
| Poll: Which SDLC concept has most improved your coding workflow? | |
|---|---|