
CPT Coding Dictionary: Orthopedic Surgery Procedures
Orthopedic surgery coding is one of the fastest ways to lose revenue and trigger audits if your team codes from habit instead of documentation. Global periods, approach differences, implant work, arthroscopy-to-open conversions, fracture care components, and modifier misuse can turn an otherwise clean claim into denials, downcodes, or recoupments. This guide is built for coders, billers, auditors, and orthopedic practice leaders who need precision—not generic CPT definitions.
You’ll get a high-value orthopedic CPT terminology dictionary, a 25+ row coding action table, practical coding logic for common orthopedic scenarios, and case studies that show exactly where orthopedic claims break and how to prevent it.
1: Why Orthopedic Surgery CPT Coding Is High-Risk (and High-Value) for Revenue Cycle Teams
Orthopedic surgery coding sits at the intersection of procedural specificity, documentation depth, and payer scrutiny. A single missing detail—open vs arthroscopic approach, unilateral vs bilateral work, staged vs related return to OR, graft source, fracture manipulation status, or implant removal complexity—can materially change code selection and reimbursement. That is why teams who already know the basics from the medical billing dictionary common terms and definitions, medical coding compliance dictionary essential terms, medical claims submission complete terminology guide, and clearinghouse terminology guide for medical coders still struggle once they move into operative orthopedic claims.
Orthopedic claims also fail because coding teams often receive documentation that is clinically rich but billing-poor. Surgeons may describe extensive work in narrative form without clearly stating distinct procedures, laterality, staged intent, or whether debridement was excisional and clinically separate. That creates a dangerous environment where coders either undercode (revenue leakage) or infer details (compliance risk). The fix requires tighter alignment with clinical documentation improvement CDI terms dictionary, complete reference for coding query process terms, guide to electronic medical records EMR documentation terms, and complete guide to electronic health record EHR integration terms.
Another major pressure point is edits and bundling. Orthopedic surgery frequently involves multiple same-session services—imaging guidance, arthroscopy, meniscal work, ligament reconstruction, hardware removal, graft harvest, casting/splinting, and follow-up fracture care components—so payers and scrubbers aggressively apply edit logic. Without strong command of understanding coding edits modifiers complete guide, guide to claim adjustment reason codes CARCs, remittance advice remark codes RARCs comprehensive dictionary, and guide to medical coding regulatory compliance, teams spend more time appealing than preventing denials.
Finally, orthopedic surgery is revenue-sensitive because these are often high-dollar cases with implants, facility coordination, and post-op utilization implications. Coding errors here don’t just affect one line item—they distort charge capture, delay cash, inflate AR rework, and weaken audit defensibility. That’s why orthopedic coding performance should be tracked through comprehensive guide to charge capture terms, guide to medical coding revenue leakage prevention, revenue cycle metrics and KPIs terms and definitions, and understanding cost reporting in medical billing.
| Term | What It Means | Why It Hits Orthopedic Billing | Best Practice Action |
|---|---|---|---|
| Open Procedure | Surgery performed through open incision/exposure | Different CPT selection and reimbursement than arthroscopy/percutaneous work | Confirm surgeon explicitly documents approach |
| Arthroscopic Procedure | Joint procedure performed using arthroscope | Bundling rules and component edits are common | Map each arthroscopic service to compartment/structure |
| Percutaneous Fixation | Fixation through small stab incisions/imaging guidance | Often miscoded as open treatment | Audit operative note for exposure/manipulation details |
| ORIF | Open reduction internal fixation | Code selection depends on fracture site and treatment specifics | Capture exact anatomic site and fixation method |
| CRPP | Closed reduction percutaneous pinning | Can be confused with closed treatment or ORIF | Require documentation of reduction + pin placement |
| Closed Treatment | Fracture/dislocation managed without open surgery | Manipulation vs no manipulation materially changes coding | Never assume manipulation unless documented |
| Manipulation | Manual realignment/reduction of fracture/dislocation | Frequently denials if op note/ED note lacks clear statement | Query if “reduced” is implied but not explicit |
| Global Surgical Package | Includes routine pre/intra/post-op services | Major source of unbundling and post-op billing errors | Teach coders to separate routine vs unrelated care |
| Modifier 25 | Significant separately identifiable E/M same day | Overused in orthopedics around injections/procedures | Require distinct evaluation work documentation |
| Modifier 57 | Decision for surgery (major procedure) | Important for trauma and urgent operative decisions | Confirm visit documented surgical decision-making |
| Modifier 59 / X{EPSU} | Distinct procedural service modifier set | High audit focus in multi-procedure orthopedic claims | Use only with defensible documentation of distinctness |
| Modifier 50 | Bilateral procedure | Payer-specific billing rules vary; payment impact is high | Follow payer bilateral policy + laterality documentation |
| RT/LT Modifiers | Laterality identifiers right/left | Missing laterality causes denials and duplicate edits | Cross-check op note, consent, and implant log |
| Modifier 58 | Staged/related procedure during postop period | Often missed in planned reconstruction sequences | Document planned/staged intent in original op note |
| Modifier 78 | Return to OR for related procedure in postop period | Common after complications, hematoma, fixation failure | Verify unplanned return and OR setting documentation |
| Modifier 79 | Unrelated procedure during postop period | Needed when new injury/problem occurs in global | Ensure diagnosis clearly supports unrelated condition |
| Debridement (Excisional vs Nonexcisional) | Removal of tissue type/extent differs by technique | Incorrect assumptions lead to overcoding | Capture depth, tissue, tool, and purpose |
| Arthroscopy to Open Conversion | Case starts scope, then converts to open procedure | Bundling/reporting errors are common | Code final definitive work and review edit policy |
| Hardware Removal | Removal of plates, screws, rods, etc. | Separate reporting depends on site/work/documentation | Document reason, location, and distinct incision/work |
| Graft Harvest | Autograft/allograft procurement for reconstruction | Bundled vs separately reportable depends on code set | Verify graft source and payer edit rules |
| Implant Log Reconciliation | Matching implants used to documented procedure | Helps detect missed fixation/hardware services | Add implant log review to pre-bill workflow |
| Approach-Specific Documentation | Details of operative access and exposure | Distinguishes code families and complexity | Train surgeons on coding-sensitive phrases |
| Compartment-Specific Knee Arthroscopy Work | Work performed in medial/lateral/patellofemoral compartments | Separate reporting often depends on compartment distinction | Require compartment documentation in op report |
| Fracture Care Includes Follow-up | Certain fracture codes include routine follow-up care | Creates duplicate billing risk for routine visits | Differentiate routine follow-up from unrelated E/M |
| Casting/Strapping Supply vs Application | Procedure application may differ from supply billing rules | Common office billing confusion and denials | Document application type and payer supply policy |
| Medical Necessity for Repeat Procedure | Clinical support for revision/repeat intervention | High scrutiny in payer review and appeals | Tie symptoms, imaging, and failed treatment to necessity |
| Revision Surgery | Repeat/reconstructive procedure after prior surgery | Code choice and modifier use depend on indication and timing | Capture cause of failure and prior procedure details |
| Intraoperative Imaging Guidance | Fluoro/other imaging used during surgery | Often bundled; improper separate billing is common | Check CPT parenthetical/bundling guidance before reporting |
| Assistant Surgeon Modifiers | Indicate assistant physician/non-physician role | Payer edits and eligibility vary by code | Verify assistant-eligible CPT list and op note support |
| Documentation Query Trigger | Standard threshold for coder clarification requests | Prevents assumption-based coding in complex procedures | Define mandatory triggers for approach/laterality/global/modifiers |
2: Orthopedic CPT Coding Dictionary — The Terms That Most Often Change Code Selection, Modifiers, and Payment
A strong orthopedic coder thinks in decision points, not just code descriptions. The practical question is not “what procedure happened?” but “what documentation fact changes the CPT family, modifier logic, or bundling outcome?” That decision-point mindset is what separates clean claims from expensive rework. Teams should reinforce it with medical coding audit terms comprehensive dictionary, guide to fraud waste and abuse FWA terms for coders, medicare documentation requirements for coders, and medical necessity criteria essential coding guide.
1) Approach terminology: open vs arthroscopic vs percutaneous
This is the first major driver of CPT selection in orthopedic surgery. Coders cannot assume approach based on incision size or instrument names. Surgeons may use “mini-open,” “percutaneous-assisted,” or “arthroscopy-assisted” language that requires careful reading before code assignment. If the approach is unclear, query early instead of choosing the closest code and hoping edits pass. Operationally, this aligns with complete reference for encoder software terms, guide to coding software terminology, medical billing practice management systems terms defined, and guide to revenue cycle management software terms.
2) Fracture care language: with manipulation vs without manipulation
In orthopedic trauma coding, this single phrase can change reimbursement and audit outcome. Many records say “fracture reduced” or “alignment improved” without explicitly stating manipulation. Coders should not infer a manipulation when documentation is vague. This is where disciplined query processes protect both revenue and compliance, especially when claims later face scrutiny through guide to financial audits in medical billing, guide to medical coding regulatory compliance, CARCs dictionary, and RARCs dictionary.
3) Orthopedic modifiers are not “cleanup tools”
A common failure pattern is coding the primary procedure first and then using modifiers to force claim acceptance. In orthopedics, modifiers must reflect the clinical truth and billing context: laterality, staged return, related return to OR, unrelated procedure in global, bilateral work, or distinct procedural services. Modifier misuse is one of the fastest ways to attract payer edits, downcoding, and audit flags. Coders should master this alongside understanding coding edits modifiers complete guide, medical coding compliance dictionary essential terms, coding compliance trends staying ahead in a rapidly changing environment, and how new healthcare regulations will impact coding careers.
4) Global period logic changes post-op billing behavior
Orthopedic practices leak money and trigger denials when front desk, surgery schedulers, coders, and billers do not share the same global-period playbook. Routine post-op care may be included, but unrelated injuries, complications requiring OR return, or staged planned procedures can be separately billable when properly documented and modified. This is where cross-functional alignment with reference understanding Medicare reimbursement fully, guide to physician fee schedule terms, future of Medicare and Medicaid billing regulations what coders must know, and predicting changes in healthcare reimbursement models by 2027 becomes financially important.
5) Documentation granularity beats coder memory
Orthopedics has too many procedure families and payer nuances for “I’ve always coded it this way” to be safe. Great coders build a repeatable abstraction checklist: anatomic site, laterality, approach, intent, structures treated, techniques performed, implant/hardware status, distinctness, and postop/global context. That discipline reduces avoidable denials and rework while strengthening audit defensibility, especially when paired with comprehensive guide to SOAP notes and coding, guide to clinical documentation integrity terms, medical record retention and storage terms, and comprehensive guide to problem lists in medical documentation.
3: Orthopedic CPT Coding Workflow — How to Code Operative Notes Without Guessing, Overcoding, or Missing Revenue
Orthopedic surgery coding accuracy improves dramatically when teams stop “reading for story” and start “reading for coding decisions.” The operative note may be clinically excellent yet still leave key billing decisions hidden in narrative language. A structured abstraction workflow prevents both missed revenue and unsupported coding. This process also helps coders preparing for advancement through guide to CPC certified professional coder exam terms, comprehensive CCS certified coding specialist exam guide, CBCS certified billing and coding specialist exam terms explained, and medical coding certification terms dictionary.
The 9-step orthopedic operative coding sequence
Identify the primary anatomic site and laterality from the op note header and body.
Confirm procedural approach (open, arthroscopic, percutaneous, closed).
List every documented operative action (repair, reconstruction, fixation, debridement, release, removal, grafting, reduction).
Separate definitive procedures from integral steps (exposure, routine closure, standard imaging, routine debridement).
Check fracture/dislocation language for manipulation, reduction method, and fixation details.
Review hardware/implant documentation and reconcile with procedure narrative.
Assess modifier needs (laterality, bilateral, staged/related/unrelated postop, distinctness).
Validate diagnosis-to-procedure medical necessity support before final claim submission.
Trigger query if approach, laterality, manipulation status, or global-period context is unclear.
This sequence is especially effective when paired with pre-bill reviews using comprehensive guide to charge capture terms, guide to medical coding revenue leakage prevention, medical billing practice management systems terms defined, and guide to revenue cycle management software terms.
A hidden orthopedic coding failure point is copy-forward preference cards and templated op notes. Templates improve speed, but they also create contradictions (e.g., “arthroscopic portals established” in an open case template, or default bilateral text in a unilateral procedure). Coders must read for inconsistencies, not just keywords. That quality discipline is easier when teams use medical coding audit terms comprehensive dictionary, guide to financial audits in medical billing, guide to medical coding regulatory compliance, and medicare documentation requirements for coders as part of training—not just audit remediation.
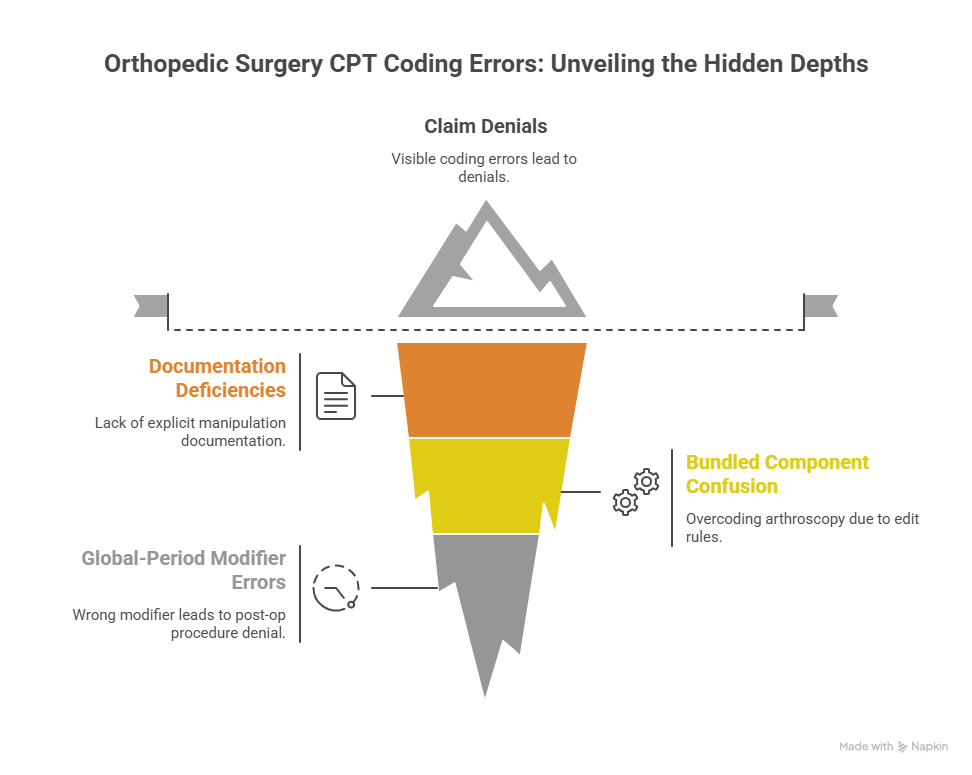
4: Case Studies — Orthopedic Surgery CPT Coding Errors That Cause Denials, Downcodes, and Audit Exposure
Case Study 1: Fracture treatment coded “with manipulation” without explicit documentation
Scenario: A patient is treated for a distal fracture in urgent orthopedics. The note documents “alignment improved after reduction maneuver,” splint applied, and follow-up arranged. The coder assigns a fracture treatment code requiring manipulation.
Risk: During payer review, the record lacks an explicit manipulation statement and procedural detail. The claim is downcoded or denied, and the practice now has to appeal with weak documentation support.
Coding lesson: Orthopedic trauma coding depends on precise fracture care language. “Reduced,” “realigned,” or “improved position” may suggest manipulation clinically, but coders should not assume procedural criteria are met without clear documentation. Build fracture-specific query triggers using complete reference for coding query process terms, medical necessity criteria essential coding guide, CARCs guide, and RARCs guide.
Best practice action: Standardize a fracture coding checklist requiring explicit documentation of manipulation status, reduction method, imaging confirmation, and follow-up care plan.
Case Study 2: Arthroscopy case overcoded due to bundled component confusion
Scenario: A knee arthroscopy includes meniscal work and chondroplasty. The operative note is detailed, but the coder separately reports services without validating compartment-level distinction and edit rules.
Risk: Claim hits NCCI/payer edits, generates denials or recoupment risk, and the practice loses time defending coding that could have been corrected before submission.
Coding lesson: In orthopedic arthroscopy, “more work documented” does not always equal “more separately billable CPT lines.” Coders must distinguish integral work from separately reportable services and anchor decisions in compartment-specific documentation. This is where understanding coding edits modifiers complete guide, guide to medical coding regulatory compliance, medical coding compliance dictionary essential terms, and guide to fraud waste and abuse FWA terms for coders matter in daily production.
Best practice action: Require compartment mapping in abstraction notes for all knee/shoulder arthroscopy claims before modifier decisions are made.
Case Study 3: Post-op procedure denial because global-period modifier was wrong
Scenario: A patient returns during the global period for a new orthopedic issue on the opposite limb. The practice bills the procedure without properly signaling that it is unrelated to the original surgery.
Risk: Payer treats the service as included in the original global package and denies payment. Rework follows, documentation is pulled, and cash is delayed.
Coding lesson: Global period billing is a workflow problem, not just a coder problem. Scheduling, intake, provider documentation, and coding must all identify whether the visit is related, staged, or unrelated to prior surgery. Teams should align this process using guide to physician fee schedule terms, reference understanding Medicare reimbursement fully, revenue cycle metrics and KPIs terms and definitions, and guide to medical coding revenue leakage prevention.
Best practice action: Create a global-period intake prompt and coder validation field that forces one choice: routine related, staged related, unplanned OR return related, or unrelated new condition.
5: Building an Orthopedic Surgery Coding Quality System — Documentation Standards, Query Triggers, Audit Defense, and Denial Prevention
If orthopedic CPT coding quality depends on one senior coder “knowing all the tricks,” your process is already at risk. Orthopedics changes too fast across payer policies, modifier edits, and practice expansion for memory-based coding to scale safely. The durable solution is a formal orthopedic coding quality system built around documentation standards, specialty-specific query triggers, pre-bill edits, and denial feedback loops. Teams can structure this work using medical coding audit terms comprehensive dictionary, guide to financial audits in medical billing, guide to medical coding regulatory compliance, and medical coding compliance dictionary essential terms.
Start with orthopedic documentation minimums for coding-sensitive procedures. Surgeons do not need to write “for coding,” but they do need a standardized set of fields that reduce ambiguity: laterality, exact anatomic site, approach, structures treated, fracture/dislocation manipulation status, fixation method, implant/hardware details, distinct procedures, and postop plan context. This can be reinforced through clinical documentation improvement CDI terms dictionary, guide to clinical documentation integrity terms, guide to electronic medical records EMR documentation terms, and comprehensive guide to SOAP notes and coding.
Next, build a specialty query matrix. Generic CDI query rules are not enough for orthopedics. Your mandatory query triggers should include: unclear approach, missing laterality, ambiguous manipulation wording, unclear staged intent for planned returns, contradiction between op note and implant log, and vague debridement documentation that lacks tissue/depth/technique. Coders should use complete reference for coding query process terms, medicare documentation requirements for coders, medical necessity criteria essential coding guide, and guide to fraud waste and abuse FWA terms for coders to keep queries compliant and focused.
Then connect coding quality to actual money and operational pain. Orthopedic leads should track denial categories by procedure family, modifier-related denials, post-op global denials, downcodes, appeal success rate, first-pass acceptance, coder query rate, and charge lag from surgery date to submission. That KPI discipline belongs in the same conversation as revenue cycle metrics and KPIs terms and definitions, comprehensive guide to charge capture terms, guide to medical coding revenue leakage prevention, and understanding cost reporting in medical billing—not isolated in a coding QA spreadsheet no one reviews.
Finally, invest in coder capability for the next five years. Orthopedic coding will be increasingly assisted by automation, encoder logic, and predictive denial tools, but specialty judgment will remain the differentiator. Coders should continue learning through medical coding education accreditation terms, understanding continuing education units CEUs for coders, understanding computer assisted coding CAC terms, and understanding medical coding automation terms AMBCI, while leaders track the bigger shifts through AI in revenue cycle management upcoming trends for medical coders, future skills medical coders need in the age of AI, how automation will transform medical billing roles by 202, and the future of medical coding with AI what to expect by 2030.
6: FAQs — CPT Coding for Orthopedic Surgery Procedures (Practical, Audit-Safe Answers)
-
One of the most expensive mistakes is coding from surgeon intent instead of documented procedural facts—especially around approach (open vs arthroscopic/percutaneous), fracture manipulation status, and modifier use in global periods. Orthopedic claims often look “close enough” until payer edits or audits expose missing documentation support. Strengthen review workflows with edits/modifiers guidance, medical coding audit terms, regulatory compliance guide, and CARCs guide.
-
No—coders should not infer manipulation based on outcome language alone. “Alignment improved” or “fracture reduced” may describe a clinical result without documenting the exact procedural method needed for specific coding. When manipulation status changes CPT selection, query the provider. This protects against denials and recoupments and aligns with coding query process terms, medical necessity criteria guide, financial audit terms guide, and FWA terms for coders.
-
Because global-period billing is a team workflow issue, not just a coder issue. If scheduling, intake, and provider notes don’t clearly identify whether the postop encounter is routine related care, a staged related procedure, an unplanned return to OR, or an unrelated new condition, the coder is forced to reconstruct context late. Fix this using shared workflows informed by physician fee schedule terms, Medicare reimbursement reference, revenue leakage prevention guide, and RCM KPIs terms.
-
Use a compartment/structure-based abstraction method before code assignment and modifier decisions. More documented work does not automatically mean more separately reportable CPT lines. Coders need to separate integral work from distinct services and then validate bundling edits. This is where edits/modifiers guide, medical coding compliance dictionary, medical claims submission terminology guide, and RARCs guide are highly practical.
-
At minimum: unclear approach, missing laterality, vague fracture manipulation language, uncertain staged postop intent, contradiction between operative narrative and implant log, unclear debridement depth/tissue/technique, and unsupported modifier distinctness. A specialty-specific trigger list reduces assumption-based coding and speeds appeals because the chart is cleaner before submission. Build it using CDI terms dictionary, coding query process terms, EMR documentation terms, and medicare documentation requirements.
-
Track metrics that connect coding quality to money and risk: modifier-related denial rate, arthroscopy edit denials, global-period denials, downcode frequency, charge lag, query rate and turnaround, first-pass claim acceptance, and appeal overturn rate. Productivity alone hides the real problems. Use revenue cycle metrics and KPIs terms, charge capture terms, cost reporting terms, and predictive analytics in medical billing trends and opportunities to build a stronger orthopedic coding dashboard.