
CPT Codes for Pediatric Care: Essential Reference Guide
Pediatric coding is not “adult coding with smaller patients.” It has its own documentation traps, age-linked code logic, vaccine administration rules, preventive visit distinctions, growth/development screening requirements, and payer-specific edits that can wipe out clean claims. One missing administration code, one wrong preventive age band, or one poorly documented sick-vs-well visit split can create denials, underpayments, audit exposure, and repeat rework across the revenue cycle.
This essential reference guide is built for coders, billers, pediatric practices, auditors, and learners who need a practical, high-value framework for CPT coding in pediatric care. It focuses on coding logic, documentation strategy, denial prevention, and workflow accuracy—so your claims are not just submitted, but defensible, reimbursable, and scalable.
1) Why Pediatric CPT Coding Is High-Risk (and Why Small Errors Cost Big)
Pediatric coding looks simple on the surface because many visits seem routine—well checks, immunizations, sick visits, screenings, and follow-ups. In reality, pediatric claims are often dense with coding layers: E/M, vaccine product codes, vaccine administration codes, counseling distinctions, screening services, preventive medicine services, developmental/behavioral assessments, and modifier use. If your workflow treats these as “quick claims,” denials pile up fast.
The first pain point is visit-type confusion: teams document a preventive visit and a problem-oriented visit in the same encounter, but fail to support both correctly. That creates edit denials, downcoding, or lost revenue. Build stronger fundamentals with AMBCI resources on medical claims submission terminology, medical billing dictionary common terms, coding edits and modifiers, and revenue leakage prevention.
The second pain point is immunization coding breakdown. Pediatric practices often lose money not because they missed the vaccine product, but because they missed the correct administration logic, counseling status, component counting (when applicable), or payer-specific billing expectations. This is where coder-biller alignment matters. Pair pediatric CPT workflows with clearinghouse terminology, charge capture terms, practice management systems terminology, and RCM software terms.
The third pain point is documentation insufficiency. Pediatric clinicians may provide excellent care but chart in a way that does not support code selection, especially for time-based counseling, behavioral screening, developmental testing, prolonged discussion, or problem-oriented work performed during preventive encounters. Tighten this area using clinical documentation improvement (CDI) terms, guide to clinical documentation integrity terms, coding query process terms, and EMR documentation terms.
The fourth pain point is payer edit friction, where the code set may be clinically appropriate but fails due to bundling edits, modifier misuse, diagnosis linkage gaps, or age-policy mismatches. To prevent expensive rework, pediatric teams should train with CARCs, RARCs, EOB interpretation, and revenue cycle metrics/KPIs.
Finally, pediatric coding is high-risk because teams often focus only on “code selection” and ignore operational sequence: scheduling template → front-desk insurance capture → nurse documentation → provider note quality → charge entry → scrubber edits → claim submission → remittance review. Pediatric practices that fix coding in isolation rarely sustain results. Connect the coding process to medical necessity criteria, medical coding regulatory compliance, guide to financial audits in medical billing, and fraud, waste & abuse terms.
2) Pediatric CPT Coding Framework: How to Code the Encounter Correctly Every Time
The fastest way to improve pediatric coding accuracy is to stop thinking in isolated code lines and start thinking in encounter architecture. Pediatric visits often contain multiple billable components, but each one depends on documentation clarity, payer policy, and sequencing. A clean pediatric claim is built in layers: visit type, problem work, procedures/tests, vaccine product/admin, screenings, and diagnosis linkage.
To support this, coding teams should standardize terminology and tools using encoder software terms, coding software terminology, EHR integration terms, and medical coding automation terms. Most recurring pediatric claim issues are workflow/system failures disguised as coder mistakes.
Here is a practical pediatric CPT framework your team can use:
Step 1: Identify the primary encounter type first
Before assigning anything else, determine whether the encounter is primarily:
preventive medicine,
problem-oriented E/M,
procedure-focused,
immunization-only,
screening-focused,
or a combined visit.
This decision controls the rest of the coding logic. If teams skip this step, they often stack incompatible services or miss reimbursable components. Reinforce foundational claim logic using medical billing dictionary terms, medical coding certification terms dictionary, CPC exam terms guide, and CCS exam guide.
Step 2: Determine whether separately identifiable problem-oriented work occurred
This is the most common pediatric revenue loss area. A child may present for a well visit, but during the encounter the provider also evaluates asthma exacerbation, otitis media, rash, constipation, ADHD medication issues, or another acute/chronic problem. If the provider performed distinct problem-oriented work and documented it clearly, it may be separately billable (subject to payer rules and modifier logic). If not documented distinctly, the work gets absorbed and lost.
Build this skill with coding edits and modifiers, medical necessity criteria, clinical documentation integrity terms, and coding query process terms.
Step 3: Capture immunizations in two parts—product and administration
This sounds basic, but pediatric practices routinely lose reimbursement because staff capture only vaccine products or only administration lines. Pediatric vaccine claims require disciplined reconciliation:
what was given,
how it was administered,
whether counseling criteria were met,
and whether documentation supports the administration code family.
Tie vaccine workflows to charge capture terminology, clearinghouse terms, medical claims submission terms, and revenue cycle KPI terms.
Step 4: Add screenings/tests only when documentation is complete
Pediatric practices perform many valuable screenings, but coding teams often leave money on the table because the chart lacks the standardized tool name, score/result, interpretation, or follow-up plan. A screening is not just “done”; it must be documented in a billable way. That requirement should be trained through EMR documentation terms, problem list documentation guidance, CDI terms dictionary, and medical coding audit terms.
Step 5: Validate diagnosis linkage and payer edits before submission
Pediatric claims frequently fail not because the CPT is wrong, but because diagnosis linkage is weak, age-related coverage rules are not met, or payer edits reject combinations. That is why every pediatric workflow needs a final “billing intelligence” check using CARCs, RARCs, EOB interpretation, and revenue leakage prevention.
The key operational lesson: Pediatric CPT coding is less about memorizing codes and more about building a repeatable encounter decomposition system. Teams that master encounter decomposition reduce denials, speed claim turnaround, and recover revenue that was already earned but never coded correctly.
3) Pediatric CPT Categories You Must Master for Clean Claims and Strong Payment
Pediatric coding teams do better when they organize CPT work into repeatable categories instead of chasing claim-level issues one by one. Below are the highest-impact pediatric CPT categories to master.
A) Preventive medicine services (well-child visits)
These are high-volume and highly visible, but still commonly miscoded. The biggest risks are wrong age band, incorrect patient status, and failure to distinguish routine preventive content from separately identifiable problem-oriented work. Pediatric teams should pair preventive coding training with medical necessity criteria, medical coding compliance dictionary, financial audit guide, and coding regulatory compliance guide.
B) Problem-oriented pediatric E/M services
Acute and chronic pediatric issues often require more cognitive work than the note reflects. If medication adjustments, monitoring decisions, comorbidity interactions, or parental counseling significantly affect management, documentation should show that complexity. This is especially relevant in asthma, ADHD, recurrent infections, dermatitis, GI complaints, and behavioral concerns. Sharpen E/M defensibility using SOAP notes and coding guide, EMR documentation terms, CDI query process terms, and audit terms dictionary.
C) Immunization coding and administration logic
This is the financial backbone of many pediatric practices—and one of the most commonly undercoded areas. The practice may provide and administer multiple vaccines correctly yet bill incompletely because staff workflows are fragmented across nurse intake, provider counseling, and charge entry. Solve this by building a vaccine reconciliation routine and connecting coding with charge capture terms, practice management systems terms, RCM software terms, and medical coding automation terms.
Quick Poll: What hurts your pediatric CPT claims most right now?
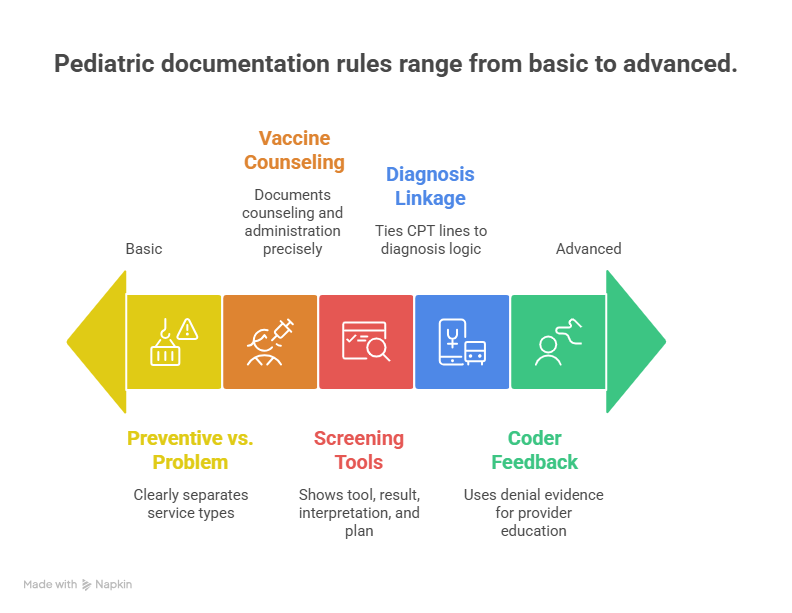
4) Documentation Rules That Make Pediatric CPT Coding Defensible
Pediatric claims are won or lost in documentation. Not because providers are careless—but because pediatric visits move fast, parents raise multiple concerns, staff touch the chart at different points, and templates often hide the details payers want. The solution is not “more charting”; it is better-structured charting that supports CPT logic clearly.
Rule 1: Separate preventive and problem-oriented work in the note
When a well-child visit also includes a medically necessary evaluation of an acute or chronic issue, the chart should clearly distinguish:
preventive services performed,
problem-oriented complaint(s),
assessment/plan for each problem,
and the additional work beyond routine preventive care.
Without this separation, coders either underbill or apply modifiers without support. Strengthen provider education with SOAP notes and coding, clinical documentation integrity terms, CDI terms dictionary, and coding query process terms.
Rule 2: Document vaccine counseling and administration workflow precisely
If the coding depends on counseling, the documentation should identify who provided counseling, that risks/benefits were discussed, and parent/guardian context where applicable. If staff administer vaccines, the clinical and charge workflows must still reconcile. Audit failures in pediatric vaccination often trace back to “assumed counseling” and missing administration capture. Support this process through medical coding audit terms, charge capture terms, clearinghouse terminology, and medical claims submission terms.
Rule 3: Screenings must show tool + result + interpretation + next step
Pediatric screening services are frequently left unbilled because the documentation says only “screen done” or “normal.” That is not operationally reliable. Build templates that prompt:
name of validated screening tool,
score/result,
provider interpretation,
and follow-up plan (especially if positive).
This not only improves billing—it improves clinical continuity. Integrate this with problem lists documentation guide, medical record retention and storage terms, EMR documentation terms, and EHR integration terms.
Rule 4: Tie every major CPT line to diagnosis logic that can survive payer review
Even correct pediatric CPT lines can deny if diagnosis linkage is weak or inconsistent with the service. This is especially true for screenings, tests, procedures, and problem-oriented E/M during preventive encounters. Teams should perform diagnosis-linkage QA using medical coding compliance dictionary, financial audit terms, FWA terms, and regulatory compliance guide.
Rule 5: Build coder feedback loops to providers using denial evidence, not vague reminders
Telling clinicians to “document better” does not improve pediatric claims. Show them exact patterns:
missed separation of well and sick work,
undocumented vaccine counseling,
incomplete screening result documentation,
weak problem complexity support,
or diagnosis linkage gaps causing denials.
Then connect education to CARCs, RARCs, EOB interpretation, and RCM KPI terms so providers see business impact, not just coding complaints.
5) Pediatric Coding Operations Playbook: How to Reduce Denials and Recover Missed Revenue
If you want measurable gains in pediatric collections, you need an operational playbook—not just code cheat sheets. The highest-performing pediatric teams standardize how they document, code, scrub, and review claims at the encounter level.
1. Build encounter checklists for common pediatric visit types
Create separate coding/documentation checklists for:
well-child + vaccines,
well-child + sick complaint,
sick visit + in-office testing,
chronic follow-up (e.g., ADHD/asthma),
screening-heavy visits,
vaccine-only encounters.
This cuts missed charges and reduces “memory-based coding.” Support checklist design with practice management systems terms, RCM software terms, coding software terminology, and encoder software terms.
2. Reconcile vaccines daily—not at month-end
Daily reconciliation between clinical vaccine logs, inventory, administered products, and submitted charges is one of the fastest ways to recover pediatric revenue. Month-end reconciliation is too late; denials, missed admin lines, and documentation gaps become harder to fix. Tie this process to charge capture terms, medical claims submission terms, clearinghouse terminology, and revenue leakage prevention.
3. Audit “combined visits” more heavily than single-purpose visits
The biggest pediatric billing friction usually comes from multi-component encounters, not simple sick visits. Audit a sample of combined visits weekly and track root causes: modifier support, preventive/problem separation, missing screenings, missed vaccine admin, wrong diagnosis linkage. Standardize audit language using medical coding audit terms, financial audit guide, coding compliance trends, and upcoming regulatory changes.
4. Train for payer variation, not just CPT descriptions
Many pediatric teams know CPT intent but still struggle because plans apply preventive coverage, modifier edits, telehealth rules, and screening reimbursement differently. Build payer-specific quick references and update them regularly. This is especially important as policies evolve alongside future Medicare/Medicaid billing regulations, how new regulations impact coding careers, predicting reimbursement model changes, and value-based care coding terms.
5. Use AI and automation carefully in pediatric coding workflows
Automation can flag missing charges, reconcile vaccine documentation, and surface modifier edits—but it can also scale bad assumptions if your rules are weak. Teach coders to validate AI suggestions against documentation and payer policy. AMBCI’s future-focused resources on medical coding automation terms, AI in revenue cycle management trends, future skills coders need in the age of AI, and future billing software innovations can help practices modernize without increasing compliance risk.
6. Build pediatric coding specialists and career pathways
Pediatric coding expertise is a career advantage because it combines E/M, preventive medicine, vaccines, screenings, compliance, and payer operations. Encourage coders to build specialization while expanding long-term growth through freelance medical coding business, director of coding operations roadmap, remote/overseas medical billing specialist guide, and international medical coding consultant career roadmap.
The core truth pediatric teams need to hear: you are not losing money because pediatrics is “complicated”; you are losing money when your documentation, coding, and billing handoffs are inconsistent. Once the handoffs become structured, pediatric claims become predictable.
6) FAQs: CPT Codes for Pediatric Care (High-Value Answers)
-
A very common underpayment pattern is incomplete coding of multi-component visits—especially well-child encounters that also include vaccines, screenings, or separately identifiable problem-oriented work. Teams often bill the main visit but miss administration lines, screening services, or supported problem-oriented E/M. Improve detection using charge capture terms, revenue leakage prevention, RCM KPI terms, and EOB interpretation.
-
Potentially yes—when a significant, separately identifiable problem-oriented service is performed and fully documented beyond routine preventive care, and when payer rules allow it. The risk is not just modifier usage; the real risk is weak documentation separation. Build strong support with coding edits and modifiers, clinical documentation integrity terms, medical coding audit terms, and regulatory compliance guide.
-
Because vaccine coding is a workflow problem, not just a code-book problem. Product codes, administration codes, counseling documentation, staff workflow, and payer edits all have to align. If any one part breaks, the claim underpays or denies. Strengthen vaccine workflows with practice management systems terms, clearinghouse terminology, medical claims submission terms, and CARCs/RARCs references.
-
At minimum, build a repeatable structure that includes the validated tool used, score/result, provider interpretation, and follow-up plan/action when indicated. “Screen normal” is usually not enough for consistent billing and audit defense. Support this with EMR documentation terms, problem lists documentation guide, CDI terms, and coding query process terms.
-
Start with three high-impact fixes: (1) combined-visit documentation templates, (2) daily vaccine reconciliation, and (3) payer-edit review by denial category. These changes usually produce measurable gains faster than broad retraining alone. Track results using CARCs, RARCs, EOB guide, and revenue cycle metrics.
-
No. What high-performing pediatric coders need most is a strong framework: encounter decomposition, documentation validation, vaccine/admin reconciliation, screening support requirements, modifier/edit awareness, and payer-policy discipline. Code lookup matters—but workflow logic matters more. Build that foundation with coding software terminology, encoder software terms, medical coding education accreditation terms, and CEUs for coders.