
UB-04 (CMS-1450) Billing Form Guide & Terms Explained
The UB-04 is not just a hospital claim form. It is a revenue document, a compliance document, a medical-necessity document, and often the difference between a clean payment cycle and weeks of avoidable rework. When teams misunderstand UB-04 terminology, they do not just risk denials. They create downstream damage in reimbursement logic, payer edits, patient balance accuracy, audit defense, and appeal success.
This guide explains the most important UB-04 terms in plain, operational language for billers, coders, revenue cycle teams, and compliance-focused leaders. The goal is not to memorize labels mechanically. It is to understand how each term affects claim construction, reimbursement, edits, remits, and cash flow so your team can submit cleaner institutional claims and resolve problems faster.
1. Why the UB-04 still matters in institutional billing
The UB-04, also known as the CMS-1450, is the standard institutional claim form used by hospitals, skilled nursing facilities, home health agencies, hospices, rehab providers, and many facility-based organizations to report services and request payment. If the CMS-1500 is the language of professional billing, the UB-04 is the language of facility billing. That difference matters because facility claims reflect room and board logic, revenue codes, occurrence data, value codes, discharge status, payer sequencing, and billing periods that are far more operationally layered than many office-based claims.
A weak UB-04 process does not fail in only one place. It fails across the entire medical claims submission process, disrupts accurate medical billing and reimbursement, increases exposure to denials prevention and management, and creates confusion in payment posting and management. One wrong statement covers period, one invalid discharge status, or one unsupported revenue code can trigger claim rejection, delayed adjudication, payer requests, or incorrect patient liability.
The real challenge is that UB-04 accuracy depends on cross-functional coordination. Registration controls identifiers and insurance order. Clinical teams influence documentation depth and medical necessity support. Coding determines principal and secondary diagnoses, procedures, and sequence integrity. Billing assembles occurrence information, revenue lines, condition indicators, and payer-specific edits. Reimbursement teams then depend on that structure when analyzing claim adjustment reason codes CARCs, remittance advice remark codes RARCs, and broader revenue cycle management terms.
That is why UB-04 terminology should never be treated as rote exam vocabulary. It is operational language that drives claim acceptance, reimbursement timing, and audit defensibility. Teams that understand UB-04 terms more deeply usually also perform better in medical coding workflow, medical coding regulatory compliance, medical billing practice management systems, and revenue leakage prevention because they see the claim as a connected financial record, not just a submission screen.
2. Core UB-04 form terms every billing team must understand
The first term every institutional billing team must master is Type of Bill, often shortened to TOB. This code does more than identify the kind of claim being sent. It tells the payer what kind of facility is billing, what category of care the claim represents, and whether the claim is an original, interim, replacement, or void. When teams misuse TOB logic, they create avoidable rejections, duplicate claim confusion, and corrected-claim failures. That is why TOB review should be tied directly to clearinghouse terminology, billing software workflows, coordination of benefits definitions, and commercial insurance billing terms.
The next term is statement covers period. This seems like a date field, but operationally it is far more than that. It controls the billing span, impacts overlap edits, influences length-of-stay reviews, and supports the payer’s understanding of when services occurred. In institutional billing, a wrong through date can derail timely filing, cause duplicate appearance, or create a false mismatch with occurrence spans and service lines. Teams that treat it casually often create rework that surfaces later in reimbursement analysis, claim reconciliation, RCM metrics and KPIs, and mastering revenue cycle management.
Then comes revenue code, one of the defining concepts of the UB-04. Revenue codes describe the category of charge being reported on a line, such as room charges, emergency services, therapy, pharmacy, supplies, or other ancillary activity. They help the payer interpret the facility service at the line level and often work in combination with HCPCS or CPT information when required. Revenue code logic is where chargemaster accuracy, service mapping, and payment policy intersect. If the revenue code is wrong, even a valid diagnosis and valid procedure can be interpreted incorrectly. That is why UB-04 proficiency depends heavily on charge capture terms, coding edits and modifiers, radiology billing terms, and lab and pathology coding essentials.
Another essential term is condition code. A condition code signals that a special claim circumstance exists. It does not replace documentation, and it does not excuse weak billing logic, but it can explain why the claim should be processed differently. Teams that misuse condition codes often either over-report them defensively or omit them when the payer actually needs the context. Both mistakes slow payment and weaken claim credibility.
Finally, teams must understand value codes, occurrence codes, and occurrence span codes as contextual reporting tools. These fields tell the payer what happened, when it happened, or what numeric value should be considered in processing. The biggest mistake is entering them mechanically without understanding why they are there. On a UB-04, context fields are never decorative. They are often the difference between a clean claim and one that goes into a manual review black hole.
3. Diagnosis, provider, and charge terms that shape reimbursement accuracy
Institutional claims live or die on clinical and financial coherence. The payer has to see a credible relationship between the diagnoses reported, the services charged, the providers identified, the dates listed, and the claim type submitted. That is why principal diagnosis, secondary diagnoses, principal procedure, attending provider, operating provider, covered charges, and noncovered charges all deserve close attention.
The principal diagnosis is the diagnosis chiefly responsible for the admission or encounter, depending on the billing context. It is not simply the most dramatic diagnosis on the chart, and it is not always the diagnosis that consumes the most words in documentation. It is the condition that best explains why the patient required the reported care. If principal diagnosis logic is weak, the claim can fail medical necessity review, trigger coding disputes, or produce payment results that do not match service intensity. That is why coders and billers need strong grounding in clinical documentation improvement, clinical documentation improvement terms, essential guidelines for accurate clinical documentation, and medical necessity criteria.
Secondary diagnoses matter because institutional reimbursement and coverage review rarely depend on one diagnosis alone. Comorbidities, complications, chronic conditions, and treatment-relevant findings can affect severity, support resource use, and explain why ancillary services were reasonable. Weak secondary diagnosis capture leaves money behind, but unsupported diagnosis inflation creates compliance risk. The right answer is disciplined, documentation-supported completeness.
Covered charges and noncovered charges are another zone where errors quietly create patient dissatisfaction and payer friction. Covered charges are those the payer may consider under the patient’s benefit and contract terms. Noncovered charges are not automatically “bad charges”; they are charges that fall outside payable coverage under the payer’s rules. The operational risk is that many organizations classify these incorrectly, then either bill the patient too early, write off recoverable amounts, or misstate the claim financially. This is where knowledge of patient responsibility terms, EOB interpretation, CARCs, and RARCs becomes critical.
Provider identifiers are equally important. The attending provider establishes who is clinically responsible for the patient’s care direction, while the operating provider may be required when a surgical or procedural role needs to be reported. A missing or mismatched NPI can create rejection, misattribution, or payer confusion that has nothing to do with coding quality. Institutional teams therefore need tighter coordination between provider master data, registration, and billing edits than many departments realize.
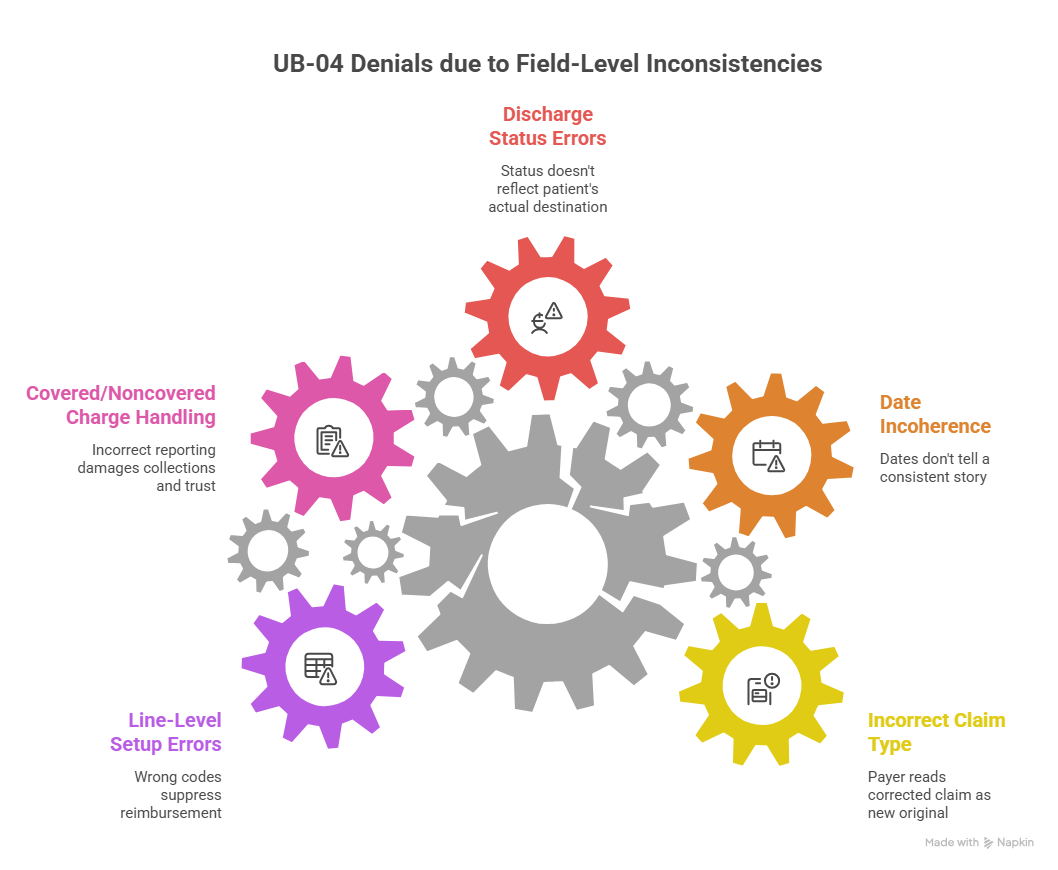
4. Field-level UB-04 mistakes that lead to denials, rework, and revenue leakage
Most UB-04 problems do not start with dramatic coding failure. They start with field-level inconsistencies that look minor during claim creation but become expensive after submission. The most common trouble spots are Type of Bill, statement covers dates, patient status, occurrence information, payer sequence, and line-level revenue code construction.
One classic failure is the corrected claim that is not truly set up as a corrected claim. Teams often know the claim needs revision, but the claim is transmitted in a way that the payer reads as a new original rather than a replacement or void. That produces duplicate logic, confusing remit activity, and unnecessary follow-up time. In high-volume settings, this mistake quietly burns staff hours while also threatening timely filing limits. It is one reason facilities need better command of claims submission process controls, clearinghouse workflow language, medical billing software terms, and revenue cycle software terminology.
Another frequent issue is date incoherence. The admission date, occurrence date, statement covers period, service line dates, and discharge status all have to tell one consistent story. When they do not, the payer sees a claim that is procedurally unstable. Even if the services were medically appropriate, the billing record becomes harder to trust. That is how organizations end up with preventable development requests, claim suspensions, or denials that seem vague but are really data-integrity failures.
Discharge status is particularly dangerous because it often affects not only payment but also downstream care-sequencing logic, especially when post-acute transfers or continuing care settings are involved. Teams sometimes default discharge status from one operational system without confirming the final patient destination. That mistake can create reimbursement distortions and post-payment vulnerability because the claim no longer reflects what actually happened to the patient.
Then there is covered versus noncovered charge handling, which is one of the fastest ways to damage both collections and trust. If a facility reports too much as covered, it invites payer reduction and rebilling complexity. If it reports too much as noncovered, it may underbill the payer or shift inappropriate liability to the patient. Either way, the organization pays for the confusion later through rework, complaints, or write-offs.
Finally, many facilities underestimate how often line-level setup causes hidden revenue leakage. The diagnosis may be right and the patient may be eligible, but a wrong revenue code, unsupported unit count, missing HCPCS detail, or flawed provider-role association can still suppress reimbursement. Facilities trying to reduce this kind of leakage usually improve faster when they combine field audits with medical coding audits, coding error rate analysis, coding denials management, and billing compliance violations review.
5. How to read UB-04 terms like a revenue cycle professional instead of a data-entry operator
The most effective institutional billers do not look at the UB-04 as a stack of boxes. They read it as a payment narrative. They ask what setting provided care, why the patient was there, what event dates shaped coverage, what services were delivered, how those services were categorized financially, who the responsible providers were, and whether the total claim tells a coherent story to the payer.
That mindset changes how staff work. Instead of only asking whether a field is populated, they ask whether it is populated correctly in relation to everything else. A strong biller reviewing a UB-04 does not just see a revenue code. They ask whether the line belongs with the diagnosis pattern, whether units make sense, whether the charge level fits the documented service, and whether a payer edit is likely. A strong reviewer does not just see a condition code. They ask why the condition exists, whether supporting documentation exists, and whether the payer will interpret the claim the same way the facility intends.
This is also why UB-04 proficiency improves reimbursement analysis after the claim is paid. When a remit shows reductions or odd patient liability, staff who understand UB-04 structure can trace the outcome back to the claim architecture much faster. They can distinguish a payer payment policy issue from a facility data issue. They can tell whether the underpayment came from coding, revenue code selection, noncovered charge treatment, discharge status, or sequencing logic. That diagnostic speed supports stronger payment posting reconciliation, better understanding of insurance adjustment codes, cleaner EHR integration workflows, and more accurate revenue cycle benchmarks.
The practical takeaway is simple: train teams to think in claim logic, not just field completion. The UB-04 is a structure of relationships. The date fields relate to the billing period. The billing period relates to the TOB. The TOB relates to frequency and care setting. The diagnoses relate to the line services. The line services relate to revenue code logic. The payer sequence relates to coverage and patient liability. When staff understand those relationships, error rates fall and appeal quality rises.
6. FAQs about the UB-04 (CMS-1450) billing form
-
The UB-04 is used for institutional or facility billing, while the CMS-1500 is used for professional billing by individual providers and many physician practices. The UB-04 is built for facility-level concepts like revenue codes, statement covers periods, Type of Bill, occurrence codes, and discharge status. The CMS-1500 is built more around professional services, provider rendering logic, and office-based claim structure.
-
Because it tells the payer what kind of institution is billing, what type of care the claim represents, and whether the submission is original, interim, replacement, or void-related. If TOB logic is wrong, the payer may reject the claim, process it incorrectly, or treat a corrected claim like a duplicate submission.
-
Revenue codes are line-level categories that identify the type of accommodation or ancillary service being billed by the facility. They help the payer interpret what the line represents financially and operationally. In many outpatient and ancillary cases, they work alongside HCPCS or CPT detail to support payment and edits.
-
There is not just one, but date inconsistency is among the most expensive because it affects statement covers periods, occurrence details, admission logic, discharge status, and timely filing interpretation all at once. The next most costly errors usually involve TOB misuse, payer sequencing failures, and weak line-level revenue code setup.
-
These fields provide additional context that affects how the payer should process the claim. Condition codes explain special circumstances, occurrence codes report important events tied to dates, occurrence span codes report relevant date ranges, and value codes report claim-related numeric information. They are not filler fields; they often shape payment interpretation directly.
-
Start by auditing the high-risk relationships, not just individual fields. Review TOB and frequency usage, date coherence, discharge status accuracy, revenue code-to-service mapping, covered versus noncovered charge logic, provider-role data, and payer sequence setup. Then tie those audits to denial trends, remit outcomes, and system edit rules so the organization fixes root causes instead of repeatedly correcting the same claims.