
Guide to Lab & Pathology Coding Essentials
Lab and pathology coding looks deceptively simple until denials start stacking, medical necessity edits fire, panels unbundle incorrectly, and documentation fails to support what was actually ordered, collected, performed, reviewed, and billed. This is where revenue quietly leaks. Strong teams do not treat laboratory and pathology coding as a back-office afterthought; they treat it as a precision workflow tied directly to clean claims, compliant reimbursement, and defensible audits.
If your organization struggles with mismatched orders, diagnosis-to-test conflicts, modifier misuse, duplicate billing, unclear panel logic, or payer-specific edits, this guide is built for you. It connects core lab and pathology coding principles to the broader realities of medical necessity criteria, coding edits and modifiers, revenue leakage prevention, and accurate medical billing and reimbursement.
1. Why Lab & Pathology Coding Is High-Risk, High-Impact Work
Laboratory and pathology claims sit at the intersection of physician intent, specimen handling, technical performance, interpretation, payer policy, and diagnosis support. That means a mistake can happen long before the claim is created. A vague order, incomplete encounter note, missing specimen source, unsupported diagnosis, wrong panel selection, or poor charge routing can all produce downstream denials that look like billing problems but actually began as documentation or workflow failures. Teams that understand charge capture terms, EMR documentation terms, SOAP notes and coding, and clinical documentation improvement terms catch these issues earlier.
One of the biggest pain points in lab billing is the assumption that a performed test is automatically a billable test. It is not. Billing strength depends on whether the service was correctly ordered, medically necessary, properly documented, accurately coded, compliant with payer edits, and assigned to the right place of service and billing entity. This is why professionals who study medical coding audit terms, regulatory compliance, Medicare documentation requirements, and physician fee schedule terms outperform teams that only memorize code ranges.
Another hard truth: lab and pathology denials are often low-dollar individually but devastating in aggregate. A missed diagnosis link on one chemistry test may look minor. The same failure repeated across a month of volume becomes a serious reimbursement drag. That is why top performers track revenue cycle metrics and KPIs, understand clearinghouse terminology, decode CARCs, analyze RARCs, and escalate patterns before they become normalized loss.
2. Core Lab & Pathology Coding Concepts You Must Master
The first essential concept is test identity. You cannot code accurately if you do not know whether a claim represents a single analyte, a defined panel, a pathology examination, a technical service, or a physician interpretation. This sounds basic, but many billing failures come from blurred distinctions between what was ordered, what was resulted, and what was ultimately billed. Teams that routinely review CPT coding for radiology procedures, cardiology procedure coding, emergency medicine CPT definitions, and gastroenterology CPT coding usually become better at lab/pathology logic because they stop thinking in isolated codes and start thinking in service architecture.
The second concept is diagnosis support. In laboratory billing, diagnosis specificity is not cosmetic. It is the difference between a clean claim and a denial for lack of medical necessity. A generic symptom may be enough in one payer environment and insufficient in another. That is why coders need fluency in ICD-11 coding standards, broad disease references such as respiratory disease coding essentials, neurological disorder codes, infectious disease coding, and specialty-specific diagnosis mapping like oncology coding case studies.
The third concept is component billing. Pathology services may involve specimen preparation, technical processing, and professional interpretation. If your workflow cannot separate who performed what, you create billing duplication risk or underbilling. This is where billing practice management system terms, revenue cycle management software terms, encoder software terms, and EHR integration terms become operational, not theoretical.
The fourth concept is payer logic. Many teams learn codes but ignore payer behavior. That is costly. Payers deny based on frequency, diagnosis support, duplicate logic, modifier validation, authorization requirements, and coverage rules. Coders who understand commercial insurance billing terms, coordination of benefits, EOB interpretation, and Medicare reimbursement fundamentals recover faster because they can diagnose the payer’s reasoning instead of merely reworking the same bad claim.
3. Documentation, Medical Necessity, and Edit Management That Prevent Denials
A strong lab or pathology claim begins before the specimen arrives. The ordering record must communicate why the test is clinically indicated, what is being evaluated, and which patient-specific facts justify performance. When the note only says “rule out” without specificity, or when a chronic condition is listed but not clearly tied to the current testing decision, billing teams inherit ambiguity they cannot ethically invent their way out of. This is why medical necessity guidance, query process terms, problem list documentation, and medical record retention terms matter so much.
The next denial trigger is edit failure. Panels may be billed incorrectly, repeats may lack rationale, modifier use may be sloppy, and diagnosis pointers may not map correctly to the performed tests. Fixing this requires more than a scrubber. It requires coding intelligence built into workflow design. Teams that study coding edits and modifiers, revenue cycle management terms, revenue leakage prevention, and accurate billing and reimbursement know how to build prevention, not just cleanup.
Another common pain point is ordering-provider education. Coders frequently see weak diagnosis specificity, invalid standing-order patterns, missing signatures, incomplete specimen context, or documentation that supports the visit but not the test. The answer is not constant downstream heroics. The answer is upstream alignment. Use denial feedback from CARC trends, payer explanations from RARC analysis, and operational insights from cost reporting terminology to show providers exactly where ambiguity is costing the organization money.
Quick Poll: What is your biggest lab or pathology coding pain right now?
4. Workflow Best Practices for Clean Claims, Strong Compliance, and Faster Payment
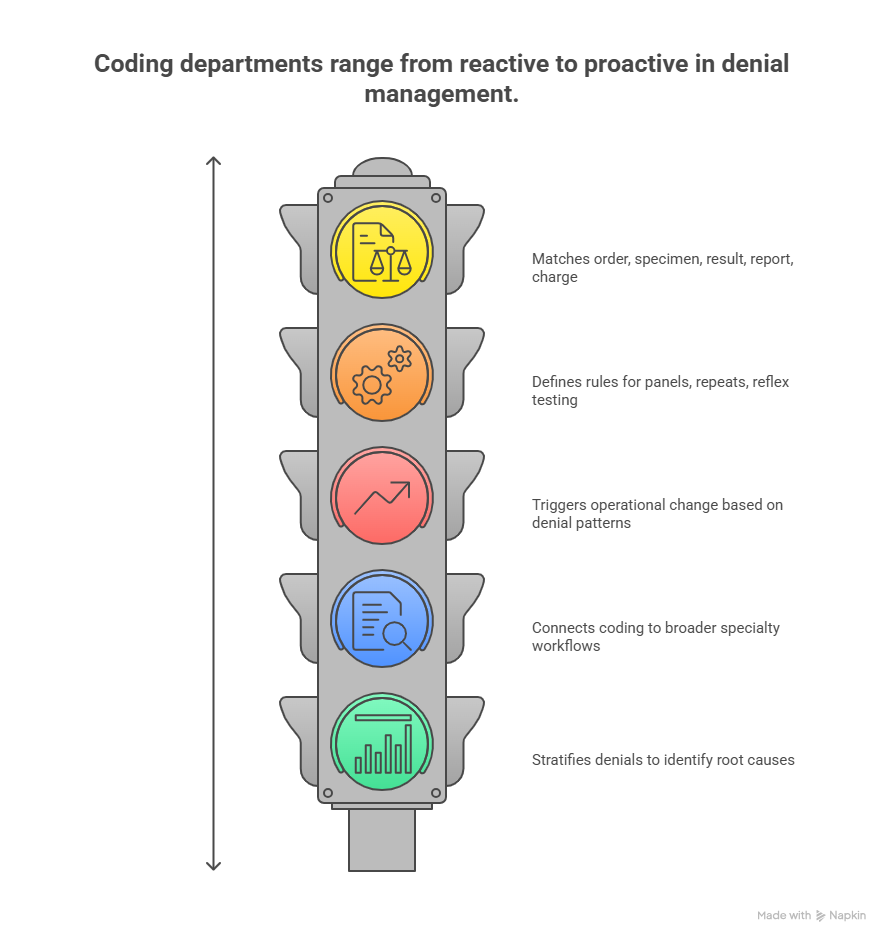
The best lab/pathology coding departments do three things exceptionally well: they reconcile, standardize, and escalate. Reconciliation means matching order, specimen, result, report, and charge so nothing is billed that lacks support and nothing supported goes unbilled. Standardization means defined rules for panels, repeats, reflex testing, send-outs, components, and payer-specific edits. Escalation means denial patterns trigger operational change instead of endless rework. These habits become easier when teams understand medical coding automation terms, future workflow shifts discussed in AI in revenue cycle management, and practical readiness topics like future skills coders need in the age of AI.
Another best practice is specialty-aware coding review. Lab and pathology do not operate in a vacuum. Their necessity and documentation often connect to broader specialty workflows. A pathology claim tied to oncology, infectious disease, allergy, dialysis, infusion, or emergency care can inherit the strengths or weaknesses of those surrounding records. That is why coders benefit from cross-training in allergy and immunology coding, dialysis coding terms, infusion and injection therapy billing, and even transport-linked workflows such as ambulance and emergency transport coding when services are part of broader episodes of care.
The smartest organizations also build dashboards that separate denial noise from denial intelligence. They do not just measure total denials. They stratify by test category, payer, ordering source, diagnosis mismatch, modifier issue, frequency edit, and documentation deficiency. This connects coding performance to revenue cycle KPIs, broader value-based care coding terms, and long-term strategy topics such as upcoming regulatory changes affecting medical billing and the future of Medicare and Medicaid billing regulations.
5. How to Build Real Expertise in Lab & Pathology Coding
Real expertise does not come from memorizing code descriptions. It comes from pattern recognition across documentation, test logic, payer edits, and reimbursement outcomes. Start by strengthening your foundation in medical coding certification terms, CBCS exam terminology, coding credentialing organizations, and continuing education units for coders. That gives you structure. Then sharpen your applied judgment through specialty dictionaries, denial trend reviews, and audit feedback loops.
You also need systems literacy. A coder who understands the payer but not the platform will still miss revenue. Learn how claims move through the clearinghouse, how documentation enters the EMR, how interfaces affect EHR integration, and how logic is applied inside encoder software. Lab and pathology accuracy improves dramatically when coders can trace where the data broke.
Finally, build the habit of reading adjacent topics because the strongest coders are never siloed. Review regulatory compliance trends, understand how automation will transform billing roles, and follow predictive analytics in medical billing. Lab and pathology coding is becoming more data-driven, more policy-sensitive, and less forgiving of weak workflow design. The professionals who thrive are the ones who can translate detail into action.
6. FAQs About Lab & Pathology Coding Essentials
-
The most common reason is failed medical necessity support. The test may have been clinically reasonable, but the documented diagnosis, indication, or diagnosis pointer does not sufficiently justify the billed service for that payer. Strengthen intake rules, diagnosis specificity, and order validation by using principles from medical necessity criteria, Medicare documentation requirements, and accurate reimbursement workflows.
-
Because panels are easy to misbill. Teams may unbundle component tests, bill duplicates, or overlook payer-specific rules for what qualifies as a panel versus separate services. Control this risk by mastering coding edits and modifiers, improving charge capture accuracy, and trending denials through revenue cycle KPI review.
-
They should verify the trigger logic, timing, documentation, and payer rules before assuming the additional service is billable. Reflex testing needs a defensible clinical or protocol-based pathway. Repeat testing needs a clear reason it was medically necessary and not accidental duplication. This is where audit terminology, query process guidance, and revenue leakage prevention become practical tools.
-
Review who performed the technical work, who issued the interpretation, whether the final report is signed, and whether the billing entity has the right to submit each component. Mistakes here cause duplicate billing, underbilling, and audit exposure. Supporting knowledge from physician fee schedule terms, practice management systems, and RCM software workflows helps coders make the correct split.
-
Move denial prevention upstream. Standardize order entry, tighten diagnosis capture, enforce documentation requirements, reconcile specimen-to-charge workflows, and teach providers what billing actually needs. Then use CARCs, RARCs, clearinghouse terminology, and compliance strategy to find the true breakpoints.
-
Yes, especially for coders who like detail-heavy, policy-sensitive work tied to clinical logic and reimbursement performance. It rewards people who can connect documentation, system workflows, payer edits, and audit defensibility. To grow faster, combine specialty skill with broader learning in medical coding education and accreditation, future coding skills, and even career strategy resources like the roadmap to director of coding operations.