
Telemedicine Coding Terms & Definitions Explained
Telemedicine coding is one of the fastest places for revenue to break, compliance risk to grow, and payer confusion to quietly drain collections. The service may be clinically appropriate, fully documented, and properly delivered, yet the claim still fails because the wrong place-of-service logic was used, the virtual modality was mislabeled, the practitioner type was mismatched, or payer-specific telehealth rules were never built into workflow. That is why telemedicine coding cannot be treated as a simple extension of in-person billing.
For coders, billers, auditors, and practice leaders, telemedicine is really a rules engine disguised as a patient encounter. You need fluency in modifiers, synchronous versus asynchronous logic, audio-only rules, platform documentation, state and payer variation, and downstream reimbursement behavior. This guide breaks the topic down into the terms that matter most, while connecting them to regulatory compliance, accurate reimbursement, revenue leakage prevention, and revenue cycle management terms.

1. Why Telemedicine Coding Breaks So Easily
Telemedicine claims do not usually fail because the coder forgot a basic definition. They fail because virtual care adds layers of logic that are not visible in a standard charge ticket. You are not just coding a service. You are coding the relationship between service type, delivery technology, patient location, provider type, documentation quality, payer rules, and reimbursement methodology. If even one layer is wrong, the claim can deny, downcode, suspend, or pay inaccurately. Teams that understand medical billing practice management systems, EHR documentation terms, EHR integration terms, and encoder software terms usually catch telemedicine errors sooner because they can see where system logic is failing.
A major pain point is false equivalence between “virtual visit” and “billable telehealth service.” Those are not the same thing. A patient portal message, brief audio check-in, remote data review, asynchronous store-and-forward interaction, and live video evaluation may all look like telemedicine to operations staff, but they often follow very different coding, modifier, and coverage rules. When organizations fail to define those distinctions clearly, front-end staff schedule the wrong visit types, providers document in the wrong templates, coders inherit ambiguity, and billing teams spend weeks fixing claims that were broken at intake. This is why charge capture terms, medical necessity criteria, problem list documentation, and SOAP notes and coding matter so much in virtual care.
Another hidden risk is payer fragmentation. Medicare, Medicaid programs, and commercial plans may use similar telehealth language but operationalize it differently. One payer may recognize an audio-only service under certain conditions, another may not. One may require a specific modifier, another may prefer place-of-service logic, and another may apply internal edits that are not obvious until remittance arrives. Coders who can interpret commercial insurance billing terms, Medicare reimbursement fundamentals, coordination of benefits, and EOB terminology are far better positioned to protect telemedicine revenue.
2. Core Telemedicine Terms Every Coder Must Understand
The first essential distinction is synchronous versus asynchronous care. Synchronous telemedicine involves real-time communication, most often audio-video, though some payer frameworks separately recognize audio-only. Asynchronous care involves information sent, stored, and later reviewed. The mistake many organizations make is flattening both into one generic “telehealth” bucket. That creates coding errors immediately because a live evaluation, a portal-based digital communication, and a later image review do not carry the same billing expectations. Teams that already understand nuanced service-type differences in radiology procedure coding, cardiology CPT coding, emergency medicine CPT definitions, and infusion billing terminology usually adapt faster to telemedicine because they already think in service architecture rather than vague labels.
The next critical terms are originating site and distant site. These sound technical, but they are operationally decisive. The originating site is where the patient is located during the encounter. The distant site is where the provider is located while delivering the service. If staff do not capture patient location at the time of care, they can inadvertently create coverage, licensure, or billing problems. A telemedicine encounter is not just about who logged into the platform. It is about where the encounter legally and financially occurred. That is why coders benefit from understanding medical record retention terms, audit terminology, Medicare documentation requirements, and physician fee schedule terms.
Place of service and modifier logic are the next major area of confusion. Many telemedicine claims fail not because the CPT or HCPCS concept is wrong, but because the claim signals the wrong context. The modifier may indicate a synchronous virtual service, while the place of service may imply something inconsistent with payer expectations. Or staff may rely on a legacy modifier that the payer no longer wants. This is why teams must stop improvising and instead maintain a payer-specific rules framework informed by coding edits and modifiers, clearinghouse terminology, claim adjustment reason codes, and remittance advice remark codes.
The last term group every coder must master involves digital service types that are not full telehealth visits. Virtual check-ins, e-visits, remote patient monitoring, and other technology-enabled services have their own initiation, time, and documentation standards. Revenue gets lost when staff either fail to capture these services or overstate them as something more comprehensive than they are. Both mistakes are costly. One is silent underbilling. The other is compliance exposure. This is where medical coding automation terms, RCM software terms, practice management system terminology, and accurate billing strategy become extremely practical.
3. Documentation, Medical Necessity, and Modifier Logic That Decide Payment
Telemedicine documentation has to do more than prove a conversation happened. It has to prove what kind of remote service happened, who delivered it, where the patient was, what technology was used, whether consent was obtained when required, why the service was medically necessary, and whether the final coded service matches the actual interaction. This is where many organizations stumble. Providers may document the clinical discussion well, yet omit the modality details that billing needs. Or they may use templated language that implies video even when the visit downgraded to audio-only because of a platform failure. Those small omissions are not small to a payer. They are the difference between a supported claim and an avoidable denial. Strengthening this area requires daily discipline around EMR documentation, CDI terminology, medical necessity standards, and query process terms.
Modifier logic is equally unforgiving. A modifier is not decorative claim data. It is a payment signal. When modifier 95, GT, or other indicators are used casually, claims can pay incorrectly or deny for reasons that feel inconsistent until you realize the payer processed the encounter under the wrong service framework. High-performing teams create explicit billing pathways for live audio-video, audio-only, portal-based, and asynchronous services. They do not ask coders to “figure it out later” from vague visit notes. They build structure into scheduling, provider templates, and charge review. That is how organizations reduce the kind of rework that burns out billing staff and quietly destroys margin. Strong control here depends on fluency in coding edits and modifiers, charge capture workflow, revenue leakage prevention, and medical coding compliance strategy.
Medical necessity in telemedicine also deserves sharper attention than it usually gets. Virtual delivery does not relax necessity expectations. A payer still wants to know why the service was needed, what was evaluated or managed, and why the billed level is justified. In fact, because some organizations assume virtual care is inherently simpler, they sometimes under-document clinical complexity and create self-inflicted downcoding. Telemedicine encounters involving chronic disease management, medication adjustments, follow-up after acute events, behavioral health issues, risk discussions, or diagnostic review can be highly substantive. But the documentation has to prove it. Coders who understand problem list strategy, medical necessity criteria, Medicare reimbursement mechanics, and value-based care coding terms are much better at protecting both payment and compliance.
Quick Poll: What is your biggest telemedicine coding pain right now?
4. Telemedicine Workflow Mistakes That Create Denials and Revenue Leakage
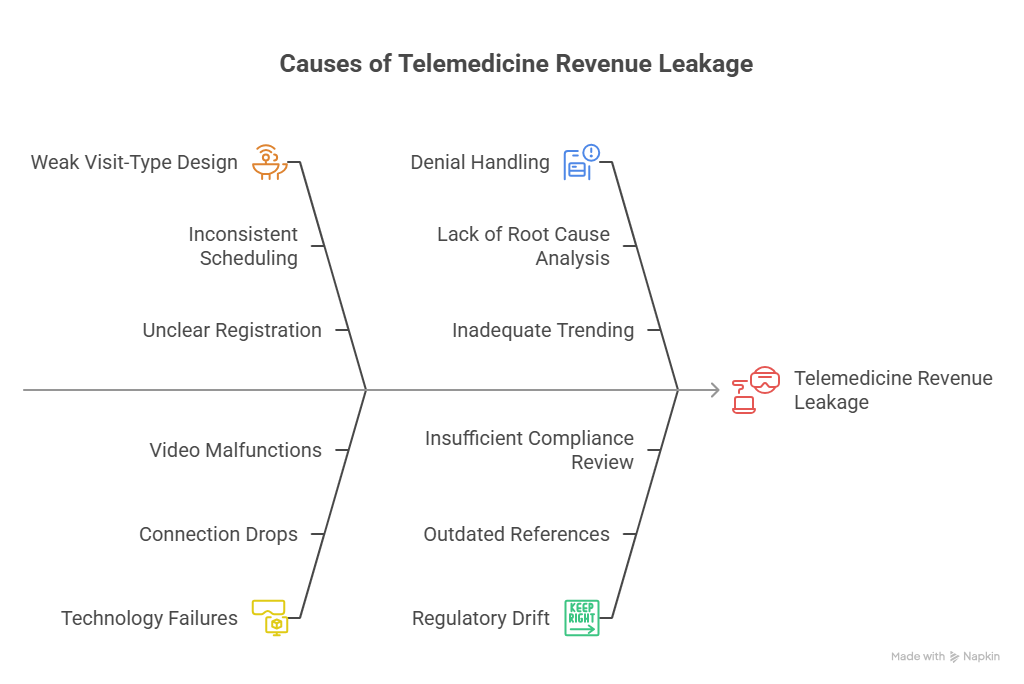
The most expensive telemedicine mistake is weak visit-type design. If scheduling, registration, and provider workflow do not distinguish between a full telehealth evaluation, a brief communication, an e-visit, and a remote monitoring interaction, coders inherit a mess that cannot be solved cleanly at claim stage. This is where organizations lose the most money: not from one catastrophic error, but from thousands of preventable mismatches between what operations thought happened and what the claim can actually support. Fixing that requires coordination across front desk, clinical, documentation, coding, and billing teams using principles from revenue cycle metrics and KPIs, revenue cycle management, practice management systems, and clearinghouse workflows.
A second major mistake is failing to capture real-world technology failures. Virtual care is messy. Connections drop. Video fails. The patient joins by phone only. The provider starts in one modality and finishes in another. If documentation still presents the encounter as uninterrupted interactive audio-video, the billing team may submit a claim that does not match reality. That mismatch is dangerous in audits and frustrating in denials because it often originates from templated language copied without scrutiny. Teams that care about defensibility train providers to document what actually occurred, not what was scheduled to occur. This is the kind of discipline reinforced by medical coding audit terms, medical record retention standards, query process guidance, and Medicare documentation expectations.
Another workflow failure is treating telemedicine denials as payer noise instead of feedback. Denials around modifier use, noncovered remote service types, missing telehealth indicators, or unsupported audio-only claims are telling you where the process broke. If billing teams only correct and resubmit without trending the root cause, the same error keeps recurring. Smart organizations map telemedicine denials by payer, service type, platform, provider template, and registration source. That turns remittance into operational intelligence. This kind of analysis depends on active use of CARCs, RARCs, cost reporting awareness, and broader billing and reimbursement strategy.
The final major mistake is underestimating regulatory drift. Telemedicine rules evolve faster than many coding teams update internal references. What worked under one policy window may later deny under another. That means telemedicine cannot be managed with static cheat sheets that never change. It needs active governance tied to compliance review, payer updates, and technology workflows. This is why coders and leaders should follow upcoming regulatory changes affecting medical billing, the future of Medicare and Medicaid billing regulations, coding compliance trends, and how new healthcare regulations will impact coding careers.
5. How to Build Real Expertise in Telemedicine Coding
The best telemedicine coders are not the people who memorize the most buzzwords. They are the people who can translate a messy virtual encounter into a defensible billing story. That requires four strengths: terminology accuracy, payer awareness, systems literacy, and denial pattern recognition. Start with strong foundations in medical coding certification terms, CBCS exam terminology, coding credentialing organizations, and continuing education units for coders. Then move quickly into telemedicine-specific application through internal audits, denial trend review, provider education, and template refinement.
Systems literacy matters especially in virtual care because encounter modality is often created or lost in technology workflows. The data might start in scheduling software, pass into a telehealth platform, sync into the EHR, and finally populate the billing system. Every handoff is a chance for the truth of the encounter to get flattened or distorted. Coders who understand EHR integration, medical billing software language, coding automation terminology, and emerging AI in revenue cycle management can troubleshoot issues that less technical coders never see.
You also build expertise by studying adjacent specialties because telemedicine is not one clinical domain. It is a delivery model. A virtual visit can involve primary care, behavioral health, chronic care, follow-up after emergency treatment, medication management, dermatology image review, or even specialty consultations tied to broader coding frameworks. Cross-training in areas like pediatric CPT coding, dermatology procedure coding, allergy and immunology coding, and medical coding audit terms makes telemedicine coding sharper because it teaches you to recognize what the clinical content of the virtual encounter is actually trying to support.
Finally, telemedicine expertise will become even more valuable as healthcare delivery grows more distributed. Remote care, digital workflows, automation, predictive analytics, and platform-driven documentation will keep reshaping billing logic. Coders who want long-term growth should study the future of medical coding with AI, future skills coders need in the age of AI, predictive analytics in medical billing, and career paths like the roadmap to director of coding operations. Telemedicine coding is not a niche anymore. It is a permanent competency.
6. FAQs About Telemedicine Coding Terms and Definitions
-
Telehealth is often used as the broader umbrella for remote healthcare-related services, while telemedicine is more commonly used for remote clinical care encounters. In day-to-day coding work, the bigger issue is not vocabulary purity but whether your organization clearly distinguishes live video, audio-only, portal-based, asynchronous, and remote monitoring services. That clarity supports documentation quality, modifier accuracy, reimbursement integrity, and compliance control.
-
Because completed care is not the same as a billable claim. Denials often happen when the wrong place of service is used, the modifier does not match payer policy, the service was audio-only but documented or billed like video, consent or patient location is missing, or the documentation does not support medical necessity. Teams reduce these denials by mastering medical necessity criteria, charge capture accuracy, CARC analysis, and RARC interpretation.
-
The biggest mistake is documenting the clinical content of the encounter without documenting the virtual delivery details billing needs. Providers often forget to note the modality used, patient location, provider location when relevant, consent, time where required, and whether technology failures changed the encounter type. Clean virtual claims depend on strong use of EMR documentation rules, CDI terms, medical record retention practices, and Medicare documentation expectations.
-
Audio-only services should never be treated as an automatic substitute for full interactive audio-video telehealth. The coder has to verify payer recognition, applicable code set, modifier or POS requirements, and whether documentation accurately reflects the actual modality used. This requires careful coordination across commercial insurance billing rules, Medicare reimbursement logic, coding edits and modifiers, and revenue leakage prevention.
-
A payer policy matrix is an internal guide showing how each payer wants telemedicine services billed, including eligible modalities, covered service types, modifiers, POS logic, audio-only recognition, and documentation expectations. Telemedicine needs this because payer variation is too great to manage from memory. Building one supports revenue cycle metrics, clearinghouse accuracy, RCM consistency, and operational reimbursement control.
-
Yes, because remote care is no longer temporary or peripheral. It is a permanent part of modern healthcare delivery, and it sits at the intersection of coding, compliance, payer behavior, technology, and documentation design. Coders who master it position themselves well for future-facing work tied to AI in coding workflows, future coder skill demands, regulatory change readiness, and leadership growth such as the director of coding operations roadmap.