
Behavioral Health Billing Terms: Comprehensive Dictionary
Behavioral health billing is where documentation nuance, payer policy, medical necessity, authorization logic, and coding precision collide. One missed distinction between psychotherapy time thresholds, crisis services, medication management, or place-of-service rules can trigger denials, underpayments, compliance exposure, and endless rework. This dictionary is built for billers, coders, auditors, and practice leaders who need operational clarity, not vague definitions. As you work through these terms, connect them with broader concepts in revenue cycle management terms, medical claims submission, denials prevention and management, and medical necessity criteria.
Behavioral health claims often fail for reasons that look small on paper but become expensive at scale: the wrong rendering provider, unsupported session length, weak treatment plan linkage, missing authorization units, or mismatched diagnosis specificity. To protect collections and reduce audit risk, teams need the same disciplined thinking used in clinical documentation integrity, coding audits, HIPAA compliance in medical billing, and accurate billing and reimbursement.
1. Why Behavioral Health Billing Vocabulary Matters More Than Most Teams Realize
Behavioral health billing punishes partial understanding. In many specialties, the work is procedure-heavy and documentation gaps are easier to spot. In behavioral health, by contrast, revenue often depends on narrative sufficiency, time rules, diagnosis support, provider type restrictions, payer carve-outs, and benefit design that varies dramatically between plans. That means a team can appear productive while silently leaking revenue through avoidable write-offs, rejections, and downcoded claims. The fix starts with language. When staff use the same definitions for authorization, episode of care, treatment plan, medical necessity, incident-to limitations, and covered service distinctions, the workflow tightens immediately.
This is especially important because behavioral health sits at the intersection of coding, billing, utilization management, and compliance. A front-desk scheduler may trigger a denial if the appointment type does not align with the authorization. A clinician may create audit risk if the note describes general stress but the billed service implies a structured therapy intervention with clear clinical purpose. A biller may post payment incorrectly if the remittance shows a behavioral health-specific edit buried in standard CARC terms and RARC definitions. A manager may misread performance if the organization lacks strong revenue cycle KPIs, clean payment posting processes, and disciplined revenue leakage prevention.
The pain point for many teams is that behavioral health denials rarely come one at a time. They cluster. Once a payer sees a pattern such as unsupported time, invalid diagnosis-to-service linkage, expired authorization, or a rendering mismatch, the backlog grows fast. Appeals become slower, staff morale drops, aging worsens, and leadership starts asking why visits are happening without cash arriving. That is why vocabulary is not academic. It is infrastructure. The more precisely your team understands terms, the faster you can align scheduling, documentation, charge capture, claim submission, denial analysis, and audit defense. Teams that want durable improvement should also strengthen their understanding of clearinghouse terminology, charge capture terms, coding edits and modifiers, and medical coding workflow terms.
2. Core Behavioral Health Billing Terms Every Coder and Biller Must Master
A behavioral health billing dictionary should start with the terms that shape claim validity before the claim ever reaches adjudication. The first is medical necessity. In behavioral health, this is not satisfied by a diagnosis label alone. The record has to show why the patient’s symptoms, functional limitations, risks, or treatment barriers justify the frequency, duration, and level of service delivered. If your notes say the patient is “doing okay” yet the claim pattern reflects ongoing higher-intensity treatment, the payer may see a disconnect and challenge coverage. That is why teams should study not only medical necessity criteria but also essential guidelines for accurate clinical documentation, SOAP notes and coding, query process terms, and EMR documentation terms.
The second cluster of terms involves service definition and coding logic. Psychotherapy, group therapy, family therapy, crisis services, medication management, and telebehavioral health are not interchangeable labels. Each implies different documentation expectations, time thresholds, provider qualifications, and payer edits. One of the most expensive habits in behavioral health billing is coding from the schedule template rather than from the actual service rendered and documented. A 60-minute slot on the calendar does not prove a 60-minute psychotherapy service occurred. A telehealth visit is not billable correctly unless the modality, provider, place-of-service logic, and modifier requirements align. Teams that struggle here benefit from strengthening broader coding knowledge in CPT coding guides, telemedicine coding, coding edits and modifiers, and EHR integration terms.
The third cluster centers on payer control terms such as eligibility verification, prior authorization, benefit limits, carve-outs, coordination of benefits, timely filing, and parity. These are the terms that quietly undermine collections when workflows are fragmented. Behavioral health is notorious for carve-out arrangements in which the medical plan is visible at registration, but the actual behavioral health administrator sits elsewhere. That creates a trap: the visit happens, the claim is sent, the denial returns weeks later, and now staff are forced into retroactive damage control. The same happens when authorization is attached to the wrong provider, wrong location, wrong code family, or wrong unit count. High-performing teams fight this by integrating commercial insurance billing terms, coordination of benefits, practice management systems terms, and RCM software terminology into daily operations rather than treating them as back-office afterthoughts.
3. Terms That Commonly Trigger Behavioral Health Denials, Delays, and Recoupments
If you want to know where behavioral health revenue breaks, follow the terms that repeatedly appear in denial work queues. Authorization is near the top. Many organizations think they have an authorization problem when they actually have a data integrity problem. The auth exists, but it is tied to the wrong CPT family, wrong servicing provider, wrong dates, or wrong unit structure. By the time the denial is visible, the visit is old, the payer is rigid, and the appeal window is already shrinking. That is why authorization should be treated like a living operational asset, not a static approval number. It needs active governance, just like revenue cycle metrics, billing software selection, payment posting management, and claims submission workflows.
Another expensive term is rendering provider. Behavioral health practices frequently employ psychiatrists, psychologists, therapists, counselors, social workers, and supervised staff under complex payer rules. When the rendering provider on the claim does not align with the credentialed clinician who performed the service, reimbursement can collapse even if the clinical work itself was appropriate. The same risk appears when a payer does not recognize a provider type for the billed code or location. This is why provider master data has to be tightly managed across the EHR, PM system, clearinghouse, and payer rosters. Teams that ignore this often blame denials on payers when the real issue is internal system misalignment. That is where understanding healthcare billing acronyms, clearinghouse terminology, encoder software terms, and coding automation terms becomes practical, not theoretical.
Then there is medical necessity, the phrase that often appears after payment rather than before it. Claims may pay initially and still be vulnerable later if the documentation does not show why the service intensity was justified. Behavioral health recoupments hurt because they force teams to defend not only coding accuracy but the clinical story itself. Was there ongoing impairment? Was the intervention specific? Did the patient’s response show active treatment rather than generic supportive conversation? Was the plan updated when progress stalled? Strong organizations defend these questions prospectively through note templates, clinician education, audit sampling, and documentation feedback loops. They do not wait for payer takebacks to discover that their records fail the standard. For stronger defense, teams should connect behavioral health billing practice with medical coding audits, coding compliance trends, billing compliance violations and penalties, and guide to medical coding regulatory compliance.
4. Documentation Terms That Decide Whether Behavioral Health Claims Survive Scrutiny
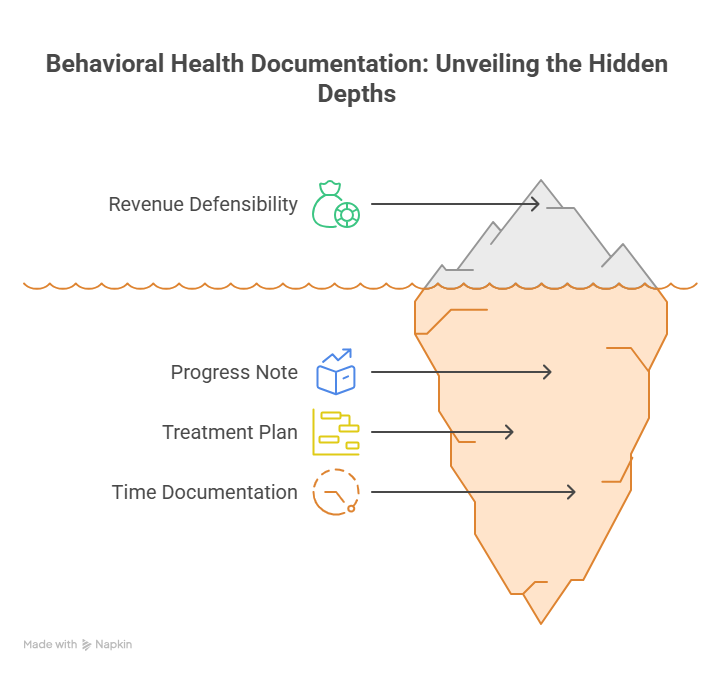
In behavioral health, documentation terms are not passive descriptors. They determine whether your revenue is defensible. Start with progress note. A progress note is not merely evidence that a patient showed up. It should show what clinical intervention occurred, how the patient presented, how the patient responded, what barriers remain, and how the service ties back to an active treatment plan. Notes that rely on vague phrases such as “processed feelings,” “support given,” or “patient stable” may feel clinically familiar, but they are often financially weak. They fail to show intervention specificity, medical necessity, and measurable therapeutic purpose. That is why many teams pair note improvement efforts with clinical documentation integrity, clinical documentation improvement terms, problem list documentation, and EHR coding terms.
Next is the treatment plan. Many organizations treat it like a compliance checkbox completed at intake and ignored afterward. That is a mistake. A treatment plan should function as the payer-facing rationale for why repeated services remain necessary. If the diagnosis remains the same but the goals, interventions, and barriers never evolve, the record starts to look templated rather than clinically responsive. Payers notice this. Auditors notice this. Plaintiffs’ attorneys notice this. In behavioral health billing, stale treatment plans undermine not only coverage but credibility. A good plan should show targeted goals, measurable markers, frequency rationale, review dates, and clear linkage to the services being billed. Teams that want more resilient documentation should also build fluency in medical record retention and storage terms, ethical practices in medical billing, accurate reimbursement guidance, and medical coding error trends.
Then comes time documentation, one of the most misunderstood documentation concepts in therapy billing. Many therapy codes depend on time thresholds, yet some notes still document only appointment length, not actual service time. Others include inconsistent time references between the schedule, note, and charge ticket. That is a denial magnet. Behavioral health billers should push for documentation that captures actual service duration, distinct therapeutic activity, and any factors affecting billable time. In telebehavioral health, this becomes even more important because payers may apply additional modality rules. A clean claim is impossible when time is ambiguous. An appeal is weak when the record looks reconstructed. The organizations that protect themselves here combine coder education, clinician training, template design, and post-bill audit review. Those same disciplines strengthen performance in coding productivity benchmarks, impact of coding accuracy on revenue, denials management analysis, and revenue cycle efficiency metrics.
5. How to Use This Dictionary to Improve Clean Claims, Collections, and Compliance
A dictionary only creates value when it changes workflow. The first operational use is cross-functional alignment. Behavioral health billing fails when scheduling, clinical staff, coders, and billers each use a term differently. If “authorization approved” means one thing to access staff, another to utilization review, and another to billing, the organization is already unstable. Build a shared glossary into onboarding, huddles, payer updates, and denial reviews. When a denial is discussed, name the failed term precisely: eligibility, carve-out, rendering mismatch, treatment plan support, timely filing, modifier logic, or medical necessity. Precision turns frustration into corrective action. It also supports stronger process design in medical billing practice management systems, revenue cycle software workflows, medical coding workflow design, and charge capture control.
The second use is denial prevention. Create denial categories that mirror dictionary terms instead of vague buckets like “payer issue” or “documentation issue.” A denial dashboard becomes far more actionable when it distinguishes expired authorization from wrong POS, invalid modifier, missing treatment plan review, noncovered service, untimely filing, COB error, or unsupported crisis criteria. This lets leadership invest in the right fix. Some problems need front-end eligibility redesign. Others need clinician education. Others need better edits in the PM system. Without term-level categorization, teams tend to throw labor at the backlog rather than remove the root cause. This is where practices should pair the dictionary with CARC guides, RARC interpretation, explanation of benefits review, and denials prevention strategy.
The third use is audit readiness. Behavioral health claims can attract scrutiny because of their reliance on narrative documentation, repeated service patterns, and medical necessity interpretation. A mature dictionary helps organizations build internal audit tools around high-risk terms: crisis billing, prolonged therapy, repeated diagnostic evaluation, telebehavioral health modifier logic, medication management by provider type, and treatment plan recertification. Audit readiness is not about making charts look better after the fact. It is about training staff to document in a way that proves the service, supports the code, and survives external review. Organizations serious about that mission should also study medical coding audit terms, Medicare documentation requirements, surgical coding compliance terms, and compliance audit trends.
Finally, use the dictionary as a training and escalation tool. New billers often memorize code ranges without understanding the operational meaning behind them. Clinicians often document clinically sound narratives without realizing which phrases weaken reimbursement defense. Supervisors often know the payer pain points but lack a structured way to teach them. A strong behavioral health billing dictionary bridges all three gaps. It gives new staff language, gives experienced staff a calibration tool, and gives leaders a framework for policy, templates, and QA. In an environment where small wording failures can destroy margin, that shared language is one of the highest-return assets a practice can build.
6. FAQs About Behavioral Health Billing Terms
-
The biggest mistake is assuming everyone understands the same term the same way. In reality, “authorized,” “covered,” “medically necessary,” “telehealth-ready,” and “billable” are often treated as synonyms when they are completely different concepts. That confusion leads to visits being scheduled under the wrong assumptions, notes being written without the right support, and claims being submitted with silent defects. Practices reduce this risk by standardizing definitions, embedding them into workflows, and tying them to denial review and staff education.
-
Because payers are not only checking whether a code exists; they are checking whether the record proves the service intensity, duration, and clinical need. Behavioral health documentation often relies on narrative language, which means vague wording can undermine otherwise appropriate care. When symptoms, functional impairment, treatment plan linkage, intervention specificity, and patient response are not clear, payers may see the record as insufficient even if the visit happened exactly as described.
-
Treatment plans act as the connective tissue between diagnosis, goals, interventions, and repeated visits. Without that linkage, ongoing therapy can look unsupported or routine rather than medically necessary. A weak or outdated treatment plan makes every subsequent note weaker because the payer cannot easily see why services continue at the documented frequency. The strongest treatment plans are specific, current, measurable, and visibly reflected in each progress note.
-
At minimum, track eligibility, authorization, carve-out/vendor routing, rendering provider mismatch, NPI mismatch, POS error, modifier error, timely filing, COB error, noncovered service, medical necessity, documentation insufficiency, and treatment plan deficiency. Generic denial buckets hide patterns. Term-level categorization shows whether the real issue is front-end intake, clinical documentation, coding logic, payer setup, or follow-up execution.
-
Because telebehavioral health requires multiple elements to align at once: payer coverage rules, service eligibility, provider type, place of service, modifier use, licensure considerations, and modality documentation. A claim can be clinically appropriate and still deny because one administrative element is off. Teams that perform well usually maintain payer-specific telehealth rules and update them aggressively instead of relying on memory or old cheat sheets.
-
Use it in four places: onboarding, denial management, documentation review, and payer policy updates. Build staff training around the highest-risk terms. Create denial categories that mirror those terms. Audit charts against those definitions. Update front-end scripts and claim edits when payer rules change. When the same language is used from scheduling through payment posting, preventable leakage drops, clean claim rate improves, and appeals become far more successful.