
Medicaid Reimbursement Rates & Calculator
Medicaid reimbursement looks simple from a distance. A code is billed, a fee schedule exists, and payment arrives. Real workflows are harsher. Rates differ by state, place of service, program structure, provider type, managed care arrangement, modifiers, documentation quality, and filing accuracy. One weak assumption can distort expected payment, trigger underpayment blindness, or create a false productivity picture across the revenue cycle.
This guide is built to fix that. It explains how Medicaid reimbursement rates work, what variables shape expected payment, how to think through a practical reimbursement calculator, and where coders and billers lose money when they rely on fee schedules without reading the operational rules around them.
1. Why Medicaid reimbursement calculations go wrong so often
Medicaid reimbursement mistakes usually start with a very human shortcut: teams treat the rate as the answer instead of treating the rate as one input. A posted fee schedule might show a payment amount, but that alone does not tell you what the claim will actually pay. Payment depends on whether the service is billed under state fee-for-service or a managed care plan, whether coordination of benefits COB clear definitions applies, whether the code is affected by understanding coding edits modifiers complete guide, whether the documentation supports medical necessity criteria essential coding guide, and whether claim construction lines up with guide to healthcare claims management terms.
Another reason calculations fail is that many teams blur the line between gross charge, allowed amount, expected payment, and collectible revenue. Those are not the same number. If a clinic bills $220 for a service and the Medicaid program allows $74, then $220 is financially meaningless for payment forecasting unless some secondary payer logic changes the picture. This is why coders and billers need fluency in commercial insurance billing terms essential guide, reference understanding Medicare reimbursement fully, guide to physician fee schedule terms, and revenue cycle management RCM terms explained. Rate literacy protects the revenue cycle from false expectations.
State-by-state variation adds another layer of risk. Medicaid is not one reimbursement universe. It is a patchwork of state policies, managed care arrangements, coverage rules, fee schedules, and payment quirks that can make two identical claims behave differently across geographies. If your estimate ignores rate effective dates, provider-type rules, place-of-service differences, or current policy bulletins, the calculator becomes a false comfort device. That is why operational teams benefit from the discipline embedded in guide to electronic data interchange EDI billing terms, clearinghouse terminology guide for medical coders, advanced guide to claims reconciliation terms, and guide to payment posting in medical billing, because accurate reimbursement forecasting requires operational follow-through, not just lookup skills.
The real goal of a Medicaid reimbursement calculator is not to guess a pretty number. It is to create a defensible expected payment model that reflects how the claim will behave in the real system. That is a different level of discipline, and it is what separates smart revenue-cycle teams from teams that keep “getting surprised” by their own payments.
| Input / Term | What It Means | Why It Changes Reimbursement | Best Practice for Calculation |
|---|---|---|---|
| State fee schedule | Published state Medicaid payment basis | Rates vary significantly by state | Always anchor estimate to current state source |
| Managed care contract | Plan-specific payment rules under Medicaid MCOs | Can differ from fee-for-service Medicaid | Separate MCO rates from state FFS assumptions |
| Fee-for-service | Direct state Medicaid reimbursement model | Often uses different pricing logic than MCO plans | Identify payer structure before estimating |
| Procedure code | CPT/HCPCS code being billed | Base driver of reimbursement | Verify exact code and version year |
| Modifier | Code addition changing service circumstances | Can alter or deny payment | Model modifier-specific reimbursement separately |
| Place of service | Location where service occurred | Some rates differ by setting | Include POS in rate lookup rules |
| Provider type | Rendering provider classification | Certain services pay differently by provider class | Confirm enrolled specialty and credential type |
| Billing provider | Entity submitting claim | Payment logic can depend on billing relationship | Check group versus individual billing effects |
| Units | Number of billable service increments | Multiplies payment amount | Validate time, quantity, and MUE-related logic |
| Rate ceiling | Maximum reimbursable amount | Can limit payment despite charges | Use lower of contracted logic and ceiling where required |
| Allowed amount | Maximum recognized payment basis | Drives actual payable amount | Do not confuse billed charge with allowed amount |
| Patient eligibility | Coverage status on date of service | Invalid eligibility can nullify payment estimate | Verify coverage for exact service date |
| Prior authorization | Required approval before service | Missing auth may reduce or deny payment | Build auth status into calculator assumptions |
| Medical necessity | Clinical justification for the service | Correct rate means nothing if support is weak | Link estimate to documentation sufficiency |
| NCCI edit | Code pair edit or unit limit restriction | May reduce line payment or deny entirely | Screen edits before projecting reimbursement |
| MUE | Maximum units allowed for a code | Caps reimbursable units | Compare billed units to allowable threshold |
| Bundling rule | Service included within another payment | Separate reimbursement may disappear | Test whether line item is separately payable |
| Capitation | Fixed plan payment model | Service-level rate logic may not apply the same way | Know whether encounter data replaces fee-based payment |
| Encounter submission | Reporting service under managed care even when fee not paid line-by-line | Important for analytics and compliance | Distinguish encounter capture from payable claim estimate |
| TPL | Third-party liability coverage ahead of Medicaid | Medicaid may pay secondary only | Adjust estimate for other payer involvement |
| COB | Coordination of benefits sequencing | Changes payable responsibility | Use primary paid amount in projection if applicable |
| Timely filing | Deadline for claim submission | Expired filing windows void expected reimbursement | Never model collectible revenue outside filing rules |
| Retro eligibility | Coverage granted after date of service | Can reopen collectible payment potential | Recalculate with retroactive coverage dates |
| Rate effective date | When the fee schedule value became active | Using wrong year produces bad projections | Match rate date to date of service |
| Policy bulletin | State or plan payment update notice | Can change rules without obvious warning | Review updates before trusting old rates |
| Denial code | Reason payment was reduced or rejected | Essential for refining calculator assumptions | Use denial trends to improve projection logic |
| Net expected reimbursement | Projected collectible amount after known payment rules | Most useful operational number | Base it on allowed logic, not posted charges |
2. The core rate variables every Medicaid calculator must include
A useful Medicaid calculator begins with the most basic but most commonly mishandled inputs: state, payer structure, code, modifier, date of service, provider type, and place of service. Miss any one of those and the estimate can drift far enough to damage budgeting, A/R planning, denial analysis, and productivity reporting. Teams should treat these inputs with the same seriousness they bring to comprehensive guide to CMS-1500 form terms and definitions, UB-04 CMS-1450 billing form guide and terms explained, medical billing practice management systems terms defined, and guide to revenue cycle management software terms, because the best reimbursement model still collapses if bad claim data feeds it.
The procedure code is the obvious centerpiece, yet even that input is often mishandled. Rates change over time. Code sets are updated. Local plan rules can change reimbursement behavior. Some services are separately payable only under narrow circumstances. Others bundle into broader payment logic. That is why coders and billers should pair procedure-level work with CPT modifiers dictionary usage and examples explained, comprehensive CPT coding guide for cardiology procedures, CPT coding reference for radiology procedures explained, and guide to preventive medicine CPT coding. The more clearly you understand the billed service, the more realistic your Medicaid estimate becomes.
Modifiers deserve special attention because they frequently determine whether a claim pays differently, pays less, or does not pay at all. A calculator that ignores modifier logic is not really a calculator. It is a partial lookup. The same applies to units. A code paid per unit can behave very differently once MUE-type restrictions, time thresholds, or bundling rules enter the picture. That is why teams often improve accuracy when they pair reimbursement modeling with guide to charge capture terms, medical coding workflow terms complete reference, guide to accurate medical billing and reimbursement, and guide to medical coding revenue leakage prevention. Revenue leakage often begins long before a denial. It starts when the estimate assumes payment rules are simpler than they are.
Provider type and payer structure are just as important. Medicaid fee-for-service, Medicaid managed care, capitated arrangements, and encounter-based reporting can all distort a simplistic payment model. If the team does not distinguish payable line-item reimbursement from encounter submission logic, the calculator can create fake revenue. That mistake shows up later in forecasting, collections, and executive reporting.
3. How to build a practical Medicaid reimbursement calculator that operations teams can trust
A practical calculator should follow a sequence rather than a single formula. First, identify the exact payer pathway: state Medicaid fee-for-service, Medicaid managed care plan, capitated contract, or another arrangement involving third-party liability and COB logic. Second, verify eligibility on the exact date of service. Third, map the billed service using code, modifier, units, provider type, and place of service. Fourth, test the line against edit logic, authorization rules, and documentation strength. Fifth, project the allowed amount. Sixth, reduce that number if any known primary payer or contractual logic changes Medicaid’s responsibility. This framework becomes far stronger when paired with explanation of benefits EOB comprehensive guide, dictionary patient responsibility and copay terms clarified, guide to healthcare claims management terms, and medical billing reconciliation terms comprehensive guide, because true reimbursement modeling must reconcile expected payment with posted payment patterns.
The most useful calculator output is not just “expected reimbursement.” It should show the assumptions underneath that number. Teams need visibility into whether the estimate assumes clean eligibility, valid authorization, no bundling conflict, valid modifier usage, collectible timely filing status, and adequate documentation. Without those assumptions, a calculator creates dangerous overconfidence. This is where medical necessity criteria essential coding guide, medicare documentation requirements for coders, guide to medical coding regulatory compliance, and complete guide to coding ethics and standards matter, even though the topic is Medicaid. A rate is only collectible if the claim is defensible.
The calculator should also be dynamic enough to learn from denial history. If a service repeatedly underpays due to missing prior authorization, bundling edits, secondary payer sequencing, or plan-specific modifier restrictions, then the calculator must incorporate that history. Otherwise, the same mistake repeats in forecasting every month. Teams that close this loop usually rely on guide to claim adjustment reason codes CARCs, remittance advice remark codes RARCs comprehensive dictionary, guide to data analytics and reporting terms for coders, and revenue cycle metrics and KPIs terms and definitions to convert payment variance into better reimbursement logic.
A good Medicaid calculator does not promise precision in every case. It gives teams a high-quality expected range, flags the conditions that could push the claim off course, and makes it easier to detect underpayments quickly. That is what operations teams can actually trust.
4. Where Medicaid reimbursement breaks down after the claim is submitted
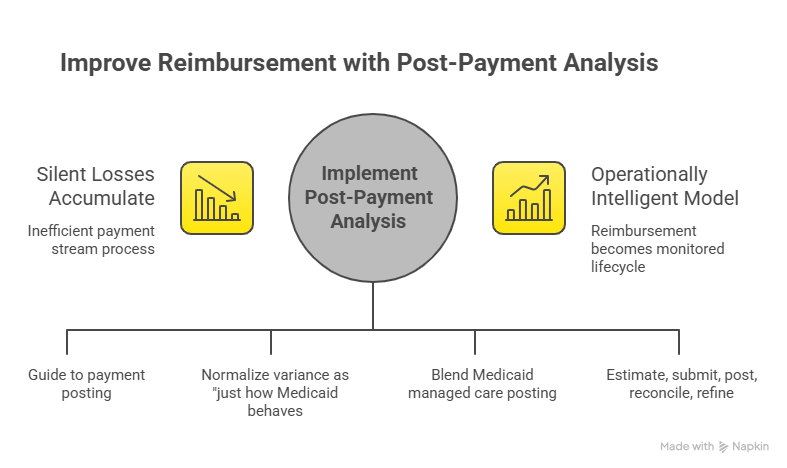
Many teams focus intensely on pre-submission rate logic and then lose discipline once the claim moves into the payment stream. That is where silent losses accumulate. A claim may pay partially, deny for an avoidable edit, get reprocessed under the wrong plan logic, or post in a way that hides underpayment across a large volume of encounters. If your process stops at claim submission, then the reimbursement calculator has no feedback loop. You need the operational visibility provided by guide to payment posting in medical billing, advanced guide to claims reconciliation terms, medical billing reconciliation terms comprehensive guide, and understanding collections and bad debt in medical billing to see whether expected payment actually converts into money.
Underpayment detection is especially weak in many Medicaid workflows because teams normalize variance as “just how Medicaid behaves.” That attitude is expensive. Some variances reflect legitimate plan logic. Others reveal rate setup errors, wrong effective dates, configuration problems in the practice management system, missing modifiers, incorrect payer sequencing, or claims that were priced under outdated rules. This is why post-payment analysis should sit next to guide to medical coding revenue leakage prevention, medical billing practice management systems terms defined, guide to revenue cycle management software terms, and understanding medical coding automation terms. Payment integrity is a systems problem as much as a coding problem.
Managed care adds another trap. Some organizations unintentionally blend Medicaid managed care posting patterns with state fee-for-service expectations in the same dashboard. That creates misleading variance reports and hides which lines are truly collectible. A reimbursement calculator should segment those worlds clearly and feed separate analytics. Otherwise leadership starts comparing unlike payment behaviors and pushing the wrong operational fixes.
The teams that perform best treat reimbursement as a monitored lifecycle. They estimate carefully, submit accurately, post rigorously, reconcile aggressively, and refine the calculator with every meaningful variance. That is how the model becomes operationally intelligent instead of decorative.
5. How accurate Medicaid reimbursement modeling improves coding, billing, and revenue-cycle performance
When reimbursement modeling is done well, it does more than help finance predict cash. It improves upstream behavior. Coders become more sensitive to documentation strength. Billers become more disciplined about modifiers, units, eligibility, and claim construction. Managers become better at spotting services that look busy on paper but consistently underperform in actual collections. In other words, a good Medicaid calculator sharpens decision-making across the workflow. That is why it connects naturally to guide to charge capture terms, medical coding workflow terms complete reference, guide to accurate medical billing and reimbursement, and guide to professional development terms in medical coding. When teams can see the financial consequence of weak claim logic, learning accelerates.
It also helps organizations identify where volume is lying to them. A code may appear productive because it is billed frequently, yet its Medicaid reimbursement may be weak after edits, plan differentials, or documentation failures are applied. Another service may look modest in volume but produce stable collectible revenue because the workflow is clean and the rate logic is well understood. Those insights emerge only when modeling is tied to guide to data analytics and reporting terms for coders, revenue cycle metrics and KPIs terms and definitions, understanding cost reporting in medical billing, and value-based care coding terms explained. Better rate intelligence produces better service-line intelligence.
Finally, strong modeling reduces friction between teams. Coding, billing, contracting, and finance often argue over payment variance because they are working from different definitions of what a claim “should” have paid. A disciplined Medicaid reimbursement framework creates shared language around allowed amount, secondary responsibility, edit-driven reductions, collectible payment, and underpayment review thresholds. Once teams agree on those definitions, problem-solving becomes faster and blame becomes less useful.
That is the real value of a Medicaid reimbursement calculator. It does not just predict money. It exposes where your workflow truly understands Medicaid and where it is still guessing.
6. FAQs
-
There is no single most important input because the estimate fails when any major variable is wrong. State, payer structure, code, modifier, place of service, provider type, units, and date of service all matter. That is why accurate modeling should sit on top of comprehensive guide to CMS-1500 form terms and definitions, UB-04 CMS-1450 billing form guide and terms explained, guide to healthcare claims management terms, and medical billing practice management systems terms defined, because clean inputs determine whether the rate logic means anything.
-
The fee schedule usually reflects a base payment framework, not the entire claim reality. Payment can change because of modifiers, bundling edits, unit limits, place-of-service rules, managed care contracts, COB, TPL, timely filing issues, prior authorization problems, or documentation weakness. To understand the gap, teams should use understanding coding edits modifiers complete guide, coordination of benefits COB clear definitions, guide to claim adjustment reason codes CARCs, and remittance advice remark codes RARCs comprehensive dictionary together rather than treating the fee schedule as the final answer.
-
Not automatically. Managed care arrangements can use plan-specific payment terms, capitation, encounter-driven reporting, or reimbursement behavior that differs materially from state fee-for-service Medicaid. Teams should separate these models operationally and analyze them through revenue cycle management RCM terms explained, guide to revenue cycle management software terms, advanced guide to claims reconciliation terms, and guide to payment posting in medical billing, otherwise the calculator will blend unlike payment logic.
-
Yes, if it is built correctly. A strong calculator can flag risky combinations involving authorization, eligibility, modifier use, bundling logic, unit limits, or secondary payer sequencing before the claim is submitted. It becomes even stronger when denial feedback is incorporated through guide to healthcare claims management terms, guide to claim adjustment reason codes CARCs, remittance advice remark codes RARCs comprehensive dictionary, and guide to medical coding revenue leakage prevention. It will not eliminate denials by itself, but it can make them more predictable and more preventable.
-
The allowed amount is the maximum recognized payment basis under the applicable rate logic. Expected reimbursement is the collectible amount you reasonably project after accounting for real-world factors such as payer sequencing, edits, prior payments, or known exclusions. That distinction becomes clearer when teams study reference understanding Medicare reimbursement fully, guide to physician fee schedule terms, explanation of benefits EOB comprehensive guide, and dictionary patient responsibility and copay terms clarified, because payment forecasting requires cleaner definitions than simple charge entry does.
-
It should be reviewed whenever fee schedules change, policy bulletins are issued, managed care contracts update, code sets change, or denial trends reveal broken assumptions. Waiting too long guarantees stale estimates and distorted forecasts. Teams that stay ahead usually tie updates to understanding medical coding system updates and releases, guide to data analytics and reporting terms for coders, revenue cycle metrics and KPIs terms and definitions, and guide to professional development terms in medical coding so the tool improves with the workflow instead of lagging behind it.