
Physician Fee Schedule Reimbursement Guide
A physician practice can code a visit correctly, document the service thoroughly, submit the claim on time, and still lose money when the team misunderstands how the Physician Fee Schedule actually shapes payment. Reimbursement rises or falls through RVU structure, place of service, modifier use, status indicators, bundling logic, and payer interpretation. Teams that want cleaner revenue need stronger command of physician fee schedule terms, Medicare reimbursement, coding edits and modifiers, and broader revenue cycle management.
This guide shows where Physician Fee Schedule reimbursement is won, where it quietly leaks, which terms actually move dollars, and how billing teams can turn payer rules into cleaner payments. The goal is practical control over claims management, charge capture, payment posting, claims reconciliation, and revenue leakage prevention before small reimbursement errors harden into monthly margin loss.
1. How the Physician Fee Schedule Actually Controls Payment
The Physician Fee Schedule shapes reimbursement long before a remittance arrives. It influences how CPT and HCPCS services are valued, how site-of-service affects payment, how modifiers change reimbursement, and how bundled logic limits what can be paid together. A team that reads only the paid amount without understanding the underlying structure stays reactive. A team that understands physician fee schedule terms, medical billing reimbursement, CMS-1500 form terms, and EDI billing terms can predict which services deserve scrutiny before cash slips away.
The fee schedule also interacts with documentation, coding, and specialty workflow in ways many practices underestimate. A service can be valued differently because of provider type, place of service, assistant surgeon rules, bilateral rules, multiple procedure reductions, or global package status. Those choices sit directly beside medical necessity criteria, clinical documentation improvement terms, SOAP notes and coding, and EMR documentation terms. When the chart, claim, and fee schedule logic do not tell the same story, reimbursement weakens fast.
Practices also lose control when they treat the Physician Fee Schedule as a coder-only or biller-only concern. It should influence front-end registration, ordering patterns, documentation habits, edit design, and denial follow-up. That is why strong organizations connect fee schedule logic to practice management systems, RCM software terms, data analytics and reporting terms, and revenue cycle metrics and KPIs instead of leaving payment interpretation to whatever arrives on the 835.
Physician Fee Schedule Terms Map: What They Mean and What You Must Do (30 Rows)
| Term | What It Means | Why It Hits Reimbursement | Best Practice Action |
|---|---|---|---|
| Work RVU | Relative value assigned to physician time, skill, and intensity | Directly shapes the professional portion of reimbursement | Review high-volume codes for wRVU-driven revenue variance |
| Practice Expense RVU | Value assigned to overhead and clinical resource cost | Site of service can reduce or raise payment materially | Audit POS selection on office and facility claims |
| Malpractice RVU | Value assigned to professional liability cost | Completes the payment formula and affects final allowed amount | Use expected reimbursement models that include all RVU components |
| Conversion Factor | Dollar multiplier applied to total RVUs | Even small changes shift annual reimbursement across thousands of claims | Update fee schedules immediately after annual changes |
| Geographic Adjustment | Regional factor applied to RVU components | Locality differences alter expected payment | Validate your locality mapping in payer setup |
| Status Indicator | Code-level payment status signal in the fee schedule | Tells staff whether a service is payable, bundled, or separately restricted | Build edit rules around status indicators for high-volume codes |
| Global Period | Post-op package window tied to surgical reimbursement | Impacts whether related services are separately payable | Train coders and billers to review post-op dates before rebilling visits |
| Bilateral Surgery Rule | Payment rule for procedures performed on both sides | Wrong modifier use leads to underpayment or denial | Audit bilateral candidates against modifier logic |
| Multiple Procedure Reduction | Payment reduction when certain procedures are billed together | High-dollar cases can lose margin if reduction logic is misunderstood | Flag multi-procedure claims for pre-bill review |
| Assistant Surgeon Rule | Payment policy for assistant-at-surgery services | Restrictions vary by code and modifier use | Check assistant eligibility before claim release |
| Incident-To | Supervision and billing rule for certain services under physician billing | Wrong use creates compliance exposure and payment risk | Validate supervision, provider enrollment, and documentation before billing |
| Split / Shared Visit | Billing policy for qualified practitioner participation in a shared service | Provider selection and documentation affect who can bill and how much | Standardize documentation templates for split/shared encounters |
| Place of Service | Location code describing where service occurred | POS changes payment rate and often changes payer expectations | Monitor office versus facility POS patterns monthly |
| Telehealth Indicator | Fee schedule signal for telehealth eligibility or restrictions | Wrong assumptions create denials or reduced payment | Keep telehealth billing matrices updated by payer and date |
| PC / TC Indicator | Professional and technical component split logic | Radiology and diagnostic services often hinge on proper component billing | Train teams on component billing before variance analysis |
| Bundled Service Logic | Payment packaging under fee schedule or edit rules | Separately billing bundled services drives denials and audit risk | Cross-check high-volume claims against bundling edits |
| NCCI Edit | Code-pair edit limiting payment for certain combinations | Improper pairings suppress reimbursement | Use modifier review protocols, not blanket rebilling |
| Modifier 25 | Indicates significant, separately identifiable E/M service | Common source of payer scrutiny and underpayment | Back up use with distinct documentation support |
| Modifier 59 / X Modifiers | Signals distinct procedural service circumstances | Incorrect use can block payment or trigger audit attention | Require encounter-level rationale before adding distinctness modifiers |
| Modifier 26 | Professional component modifier | Prevents payment confusion on diagnostic services | Align component modifiers with contractual workflow |
| Modifier TC | Technical component modifier | Needed for proper payment split on eligible codes | Confirm ownership of equipment and service delivery model |
| Allowed Amount | Maximum recognized payment amount before patient or payer adjustments | Defines the reimbursement ceiling for the claim line | Model expected payment at code and payer level |
| Limiting Charge Context | Payment boundary concept in certain reimbursement settings | Protects against misunderstanding reimbursement expectations | Train teams on payer-specific allowable logic during onboarding |
| Participating Status | Provider participation relationship affecting payment and workflow | Network status changes reimbursement pathways and patient balances | Audit enrollment and participation status quarterly |
| Non-Facility Rate | Office-based payment rate including greater practice expense | Higher or lower than facility rate depending on scenario | Match POS selection to actual care setting consistently |
| Facility Rate | Payment rate when service is delivered in a facility setting | Lower practice expense can reduce professional reimbursement | Review high-volume shifts in site of care for margin impact |
| Supervision Requirement | Rule describing required physician oversight for certain services | Weak supervision documentation can collapse payment defensibility | Build provider attestation checks into workflow |
| Frequency Limitation | Restriction on how often a code may be paid | Repeat services often hit denials even when coded correctly | Use pre-bill edit alerts for repetitive utilization patterns |
| Coverage Determination Impact | Policy layer that influences whether service is payable | Medical necessity and payer policy drive payment approval | Link coding and documentation review to payer policy updates |
| Expected Reimbursement Model | Internal benchmark built from fee schedule logic and contract behavior | Essential for underpayment detection and accurate variance review | Reconcile remits against modeled expectations every month |
2. The Fee Schedule Terms That Move Dollars the Fastest
Teams often talk about reimbursement in general language when the financial movement is actually very specific. Work RVUs, practice expense RVUs, malpractice RVUs, conversion factor shifts, geographic adjustments, and status indicators decide the baseline. Then modifier logic, place of service, bundling rules, and component billing decide whether the claim keeps that value or loses part of it. That is why fee schedule literacy has to sit beside medical coding workflow terms, coding audit terms, CPT modifier guidance, and medical coding regulatory compliance.
The most dangerous reimbursement mistakes usually come from lines that look ordinary. An office visit paired with a procedure can lose payment because modifier support was weak. A diagnostic service can underpay because the claim needed professional or technical component logic tied to radiology coding terms, lab and pathology coding essentials, or anesthesia coding terms. A surgery can look properly coded and still underperform because the global package logic or assistant rules were misunderstood. Each of those failures hits reimbursement differently, which is why one denial report never tells the whole truth.
Practices also have to understand how fee schedule logic interacts with specialty mix. A pediatric practice should watch preventive and problem-oriented combinations through preventive medicine coding and pediatric CPT references. A cardiology group should map high-volume procedures through cardiology CPT guidance. Orthopedic, dermatology, gastroenterology, emergency, and sleep medicine teams should do the same with orthopedic surgery coding, dermatology CPT essentials, gastroenterology coding, emergency medicine CPT codes, and sleep medicine billing terms. The fee schedule pays code by code, not by intention.
Another reason these terms matter is underpayment review. Many teams focus on denials while accepting partial payment as good enough. That leaves revenue buried inside supposedly clean claims. Strong reimbursement control requires fluency in EOB interpretation, CARCs, RARCs, and medical billing reconciliation. Payment that posts without challenge can still be wrong. Teams need expected reimbursement logic before they can detect quiet erosion.
3. How to Read Physician Fee Schedule Reimbursement Like an Operator Instead of a Biller on Cleanup Duty
The first step is building expected payment logic before the claim is submitted. That means mapping high-volume codes to their likely reimbursement drivers: POS, component split, modifier exposure, frequency rules, global package effects, assistant rules, and payer-specific edits. Once that structure is in place, teams can compare actual remits against realistic expectations using revenue cycle analytics, reimbursement metrics, RCM terms, and claims reconciliation terms. Without that model, staff can only react to what the payer says happened.
The second step is separating true coding issues from payment-rule issues. Some underpayments are born in the chart. Others begin in the claim build. Others happen after a payer applies a fee schedule rule differently than the practice expected. Teams should review documentation quality through problem list guidance, coding query process terms, EHR documentation terms, and CDI concepts. Then they should review claim construction through clearinghouse terminology, CMS-1500 guidance, EDI terms, and claims management terms.
The third step is operational ownership. Someone has to own fee schedule variance, modifier denial trends, POS drift, and underpayment by payer. When nobody owns those categories, the organization slowly trains itself to tolerate losses as normal friction. Better teams wire fee schedule performance into practice management systems, automation terms, encoder software terms, and health information management terms so the problem surfaces before month-end closes on bad assumptions.
Quick Poll: What is your biggest Physician Fee Schedule reimbursement pain right now?
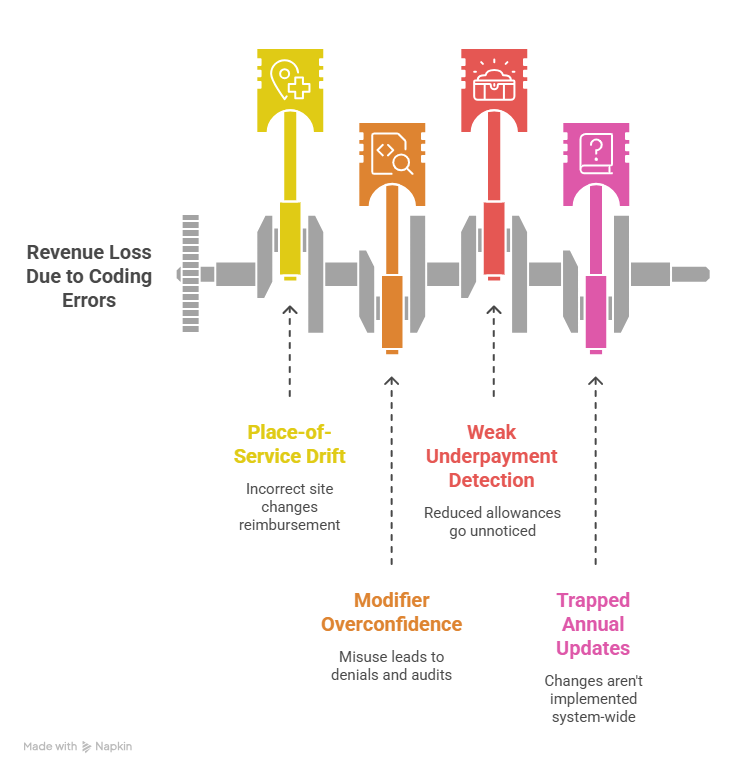
4. Where Practices Quietly Lose Money Under the Physician Fee Schedule
One major leak comes from place-of-service drift. Teams often focus on diagnosis and CPT accuracy while underestimating how site-of-service changes professional reimbursement. Office, facility, hospital, outpatient department, and telehealth settings can alter payment materially. When POS is selected casually or pulled incorrectly from the source system, the allowed amount changes before denial logic even enters the picture. That makes POS monitoring as important as charge capture controls, EMR integration terms, telemedicine coding rules, and problem list accuracy.
Another leak comes from modifier overconfidence. Teams know modifier 25, modifier 59, 26, TC, and assistant modifiers exist, but many organizations do not govern them tightly enough. One group underuses them and leaves legitimate payment on the table. Another group overuses them and invites denials, audits, or retractions. The fix lives in disciplined review of modifier guidance, coding ethics and standards, coding audit terms, and medical necessity criteria. A modifier should reflect a real payment circumstance, not a reflex added during cleanup.
Practices also lose money through weak underpayment detection. A denial gets attention because it is visible. A reduced allowance often slips through because it looks processed. That is where fee schedule education has to connect directly to EOB review, payment posting terms, CARC analysis, RARC analysis, and medical billing reconciliation. If the organization cannot compare actual payment to expected payment, it will normalize partial loss.
A final leak appears when annual updates stay trapped in a PDF, a webinar, or one manager’s memory. Fee schedule changes only matter when they are turned into system edits, coder education, front-end scripts, payer matrices, and reporting checkpoints. Practices need to operationalize them through continuing education terms, coding education and training terms, professional development terms, and coding competency assessment. Teams that fail to operationalize updates spend the next year paying for last year’s blind spots.
5. How to Build a Better Physician Fee Schedule Reimbursement Process
Start with a code-level reimbursement watchlist. Pull the highest-volume and highest-value physician services by specialty, then map the payment drivers for each. Include RVU sensitivity, POS exposure, modifier risk, global package issues, bundling exposure, component split, and payer-policy vulnerability. That turns reimbursement from a vague finance topic into an operational control framework. It also gives structure to medical coding workflow review, claims management, revenue leakage prevention, and data analytics that leadership can actually use.
Next, connect coding, billing, and posting around expected reimbursement variance. Coders should know which services attract modifier scrutiny. Billers should know which lines require fee schedule-aware review before release. Payment posters should know which variances deserve immediate escalation. Denial teams should know when a line that paid still needs follow-up. That coordination works best when practices reinforce it through RCM terms, claims reconciliation terms, practice management software concepts, and RCM software workflow. Reimbursement control collapses when each department sees only its own fragment.
Then build a monthly reimbursement review that goes beyond denial rate. Review underpayments, unexpected modifier reductions, POS shifts, component billing issues, code pair edit frequency, global period misuse, assistant billing denials, and services with repeated variance by payer. Tie that review to revenue cycle KPIs, payment posting performance, collections and bad debt exposure, and broader claims management terms. A denial dashboard alone never shows the full reimbursement picture.
Finally, turn fee schedule knowledge into durable organizational memory. Document payer quirks. Store modifier examples. Build escalation rules for underpayments. Train new staff with real variance cases. Protect that knowledge with medical record retention, healthcare data security terms, health information management practices, and disciplined coding career development. Physician Fee Schedule reimbursement gets easier when the practice stops relearning the same expensive lesson every quarter.
6. Frequently Asked Questions About Physician Fee Schedule Reimbursement
-
The Physician Fee Schedule is the payment framework that assigns value to many physician and qualified practitioner services. In daily operations, it affects expected payment, modifier behavior, component billing, site-of-service logic, and how teams model reimbursement before the remit arrives. Its practical value shows up when organizations tie it to physician fee schedule terms, Medicare reimbursement, claims management, and payment posting.
-
Underpayment can come from place-of-service errors, wrong component selection, bundling reductions, modifier issues, global period restrictions, assistant billing rules, locality issues, or payer interpretation differences. Coding accuracy matters, though reimbursement accuracy requires wider review through modifier guidance, coding edits, EOB review, and claims reconciliation.
-
Coders, billers, payment posters, denial specialists, managers, and provider-education leads should all understand it. Front-end staff also benefit when POS, provider enrollment, and documentation intake affect downstream reimbursement. That shared understanding works best when supported by practice management workflows, EMR documentation standards, problem list guidance, and coding education terms.
-
Start with a high-volume code audit. Review expected payment for your biggest physician services, then compare remits against that model. Focus on POS, modifiers, bundling, professional versus technical components, and global package issues first. That approach makes data analytics, revenue KPIs, payment posting controls, and revenue leakage review much more actionable.
-
Place of service can change practice expense valuation and alter the allowed amount. Office and facility settings often reimburse differently even when the CPT code is the same. Practices should monitor POS accuracy through CMS-1500 workflows, EMR integration, telemedicine coding terms, and claims management controls.
-
A denial is visible nonpayment or rejection. An underpayment is partial payment below what should have been allowed. Underpayments are more dangerous in some practices because they are easier to overlook. Teams need strong use of CARCs, RARCs, EOB review, and reconciliation terms to catch both.