
Medical Billing Reconciliation Terms: Comprehensive Guide
Medical billing reconciliation is where revenue cycle teams prove that every charge, every claim, every adjustment, every payment, and every patient balance actually agree across systems. It is the discipline that exposes hidden underpayments, misposted cash, avoidable denials, weak documentation, and silent revenue leakage before they become month-end surprises.
If your team understands only claim submission but not revenue cycle management terms, medical claims submission, Explanation of Benefits, payment posting and management, and revenue leakage prevention, reconciliation will always feel reactive. This guide turns the terminology into operational control.
1. What Medical Billing Reconciliation Actually Means
Medical billing reconciliation is the process of matching what should have happened financially with what actually happened. In practice, that means tying together charge capture terms, clearinghouse terminology, medical billing reimbursement principles, claim adjustment reason codes, and remittance advice remark codes so the account tells one coherent story instead of five conflicting ones.
A reconciled account answers hard operational questions quickly. Was the service documented well enough under clinical documentation integrity and essential clinical documentation guidelines? Did the diagnosis and procedure logic survive the coding workflow, the coding edits and modifiers review, the payer’s contract logic, and final payment posting? If not, reconciliation is where the mismatch surfaces.
This is why strong reconciliation sits in the middle of the full revenue cycle rather than at the end of it. It depends on clean inputs from SOAP notes and coding, stable data inside EMR documentation terms, usable diagnosis context from problem lists in medical documentation, claim transmission integrity through EHR integration terms, and rule validation through encoder software.
Most reconciliation failures are not dramatic. They are quiet. A payer pays less than expected and nobody compares it against the true allowed amount. A balance moves to patient responsibility even though coordination of benefits was wrong. A denial gets closed after a superficial review of the EOB without reading the paired RARC language. A credit balance ages because nobody mapped refund ownership inside the practice management system. Reconciliation is the control layer that stops those small misses from becoming material losses.
| Term | What It Means | Why It Matters in Reconciliation | Best Practice Action |
|---|---|---|---|
| Encounter | The patient visit or service event | Everything downstream should trace back to it | Assign a unique encounter ID and reconcile daily |
| Charge Capture | Recording billable services and supplies | Missed charges create revenue loss before claims exist | Run charge lag and missing encounter reports |
| Claim Scrub | Pre-submission validation of claim data | Bad data becomes avoidable rejections and denials | Track edit categories and root causes weekly |
| 837 Claim | Electronic claim transaction sent to payer | Submission must match posted charges exactly | Balance billed amounts against source charges |
| 999 Acknowledgment | Confirms syntactic acceptance of EDI file | Tells you whether the file structure passed | Separate syntax failures from payer logic failures |
| 277CA | Claim acknowledgment and status response | Shows whether individual claims were accepted or rejected | Work rejections before aging starts |
| Clean Claim | A claim ready for adjudication without preventable defects | Drives payment speed and lower rework | Measure clean-claim rate by payer and specialty |
| Clearinghouse Rejection | Claim stopped before payer adjudication | No true claim exists until corrected and resubmitted | Do not age as a payer denial |
| Payer Rejection | Claim refused before adjudication by payer | Blocks cash and can reset timely filing risk | Rework same day with rejection reason mapping |
| Adjudication | Payer decision on what to pay, deny, or shift | This is where expected and actual money diverge | Compare adjudication against contract expectations |
| Allowed Amount | Maximum reimbursable amount under payer rules | Foundation for identifying underpayments | Maintain payer-specific fee schedule logic |
| Contractual Adjustment | Difference between charge and allowed amount | Must not be confused with avoidable write-offs | Use payer-specific adjustment codes |
| Patient Responsibility | Coinsurance, copay, deductible, noncovered amounts | Wrong transfer creates patient dissatisfaction and bad debt | Validate against benefits and COB |
| ERA / 835 | Electronic remittance transaction | Primary source for automated posting and reason code analysis | Post with exception queues, not blind auto-posting |
| EOB | Payer explanation of how claim was processed | Useful for validating financial movement and patient liability | Match EOB detail to posted transaction lines |
| CARC | Code explaining claim adjustment reason | Separates denial, reduction, bundling, and liability causes | Map each frequent CARC to a work queue action |
| RARC | Supplemental remark explaining the payer message | Often contains the real operational clue | Never analyze CARCs without RARCs |
| COB | Rules for primary versus secondary coverage | Wrong order creates denials and patient balance errors | Reverify coverage hierarchy at registration and rebill |
| Underpayment | Payment below contractual or policy expectation | Silently drains margin if not escalated | Use expected reimbursement variance reports |
| Overpayment | Payment exceeds rightful reimbursement | Creates compliance and refund risk | Flag credits early and assign ownership |
| Unapplied Cash | Money received but not matched to accounts | Distorts A/R, payer performance, and bank reconciliation | Age unapplied cash daily |
| Recoupment | Payer recovers a prior payment | Can hit current remits and confuse variance reporting | Trace back to original claim and reason |
| Takeback | Reversal or offset tied to previous payment | Can make new claims look underpaid | Separate current adjudication from historic recovery |
| Credit Balance | Account has more credits than true liability | High compliance exposure when unresolved | Run aging and refund workflow monthly |
| Refund | Returning over-collected funds | Late refunds increase audit risk | Create documented approval path and timer |
| Posting Lag | Delay between receipt and ledger posting | Masks true cash position and follow-up priorities | Track days-to-post by payer and source |
| Expected Reimbursement | Forecast of what should be paid | Core comparator for underpayment detection | Refresh contract logic and modifier rules |
| Variance | Difference between expected and actual result | Shows where reconciliation effort must go first | Bucket by root cause, not just dollar size |
| Secondary Claim | Claim submitted to secondary payer after primary | Depends on accurate primary payment and liability posting | Do not bill secondary from assumptions |
| Rebill | Corrected or replacement submission | Poor control causes duplicate claims and duplicate payments | Use original claim cross-reference rules |
| Zero-Balance Review | Final check that the account closed correctly | Catches wrong write-offs, credits, and patient balances | Audit samples before closeout |
2. The Core Reconciliation Terms Every Medical Biller Must Master
Start with the terms that define whether money ever had a fair chance to arrive. An encounter becomes revenue only if charge capture, clinical documentation, medical necessity criteria, regulatory compliance, and the claims submission process line up. If any one of those breaks, reconciliation later becomes detective work instead of validation.
The next layer is acceptance terminology. Teams must separate claim creation from claim acceptance. A claim can be built correctly in the practice management system, mapped through RCM software terms, pushed through EHR integration, and still fail at the clearinghouse because of eligibility, subscriber, or format defects described in clearinghouse terminology. Reconciliation that ignores this distinction will incorrectly label rejections as payer denials, which distorts denial trends and staff productivity.
Then come the payment decision terms. Your team must know the difference between allowed amount, paid amount, patient responsibility, contractual adjustment, noncovered amount, and true denial. Without fluency in Medicare reimbursement concepts, physician fee schedule terms, commercial insurance billing terms, patient responsibility terminology, and accurate reimbursement rules, staff will post what the payer sent without deciding whether the payer was right.
Reason-code literacy is where reconciliation becomes operationally powerful. Teams that read only payment totals miss the actual cause of variance. CARCs explain why dollars moved. RARCs explain what the payer wants next. Denials prevention and management, coding denials management analysis, coding audits, and audit trends all become easier when reason codes are translated into specific work queues instead of generic “follow-up needed” buckets.
Finally, every biller needs balance control terminology. That includes unapplied cash, credit balance, recoupment, takeback, refund, secondary balance, and bad debt transfer. These terms sit at the intersection of payment posting, COB rules, revenue leakage prevention, RCM efficiency benchmarks, and revenue cycle metrics and KPIs. When teams get them wrong, A/R may look acceptable on paper while cash performance quietly deteriorates.
3. How Reconciliation Should Work From First Charge to Final Account Balance
A strong reconciliation workflow begins before the claim exists. First, reconcile scheduled or rendered services against captured charges. That comparison depends on charge capture controls, coding workflow terms, medical coding audit terminology, clinical documentation improvement terms, and medical record retention rules. If documentation is incomplete, services are not merely delayed; they are at risk of disappearing from revenue altogether.
Second, reconcile submitted claims against accepted claims. Many teams assume a transmitted claim is a live claim. That assumption is dangerous. You need a clean daily match between created claims, accepted claims, and rejected claims using medical claims submission steps, clearinghouse language, billing software selection logic, billing automation terms, and HIPAA compliance in billing. A claim that died at the clearinghouse should never be allowed to age like a payer-owned receivable.
Third, reconcile adjudicated claims against expected reimbursement. This is the most profitable step because it finds underpayments that standard posting misses. Build your expected logic from Medicare documentation requirements, physician fee schedule terms, commercial payer billing rules, accurate reimbursement guidance, and impact of coding accuracy on hospital revenue. When the actual payment differs, the variance needs a named cause, not a shrug.
Fourth, reconcile posted payments to bank deposits and account balances. This is where teams discover unapplied cash, split-payment errors, duplicate postings, and credit-balance risk. The workflow should pull from payment posting and management, EOB interpretation, CARC analysis, RCM benchmark reporting, and revenue leakage data. If bank reconciliation and account reconciliation live in separate silos, errors survive longer than they should.
Fifth, reconcile the final patient balance. Many organizations stop once the payer posts. That is a mistake. Patient balances must be validated against patient responsibility terms, coordination of benefits rules, denials prevention strategy, compliance violation risks, and ethical medical billing principles. Sending the wrong balance to a patient is not a minor operational error. It is a trust failure and sometimes a compliance failure.
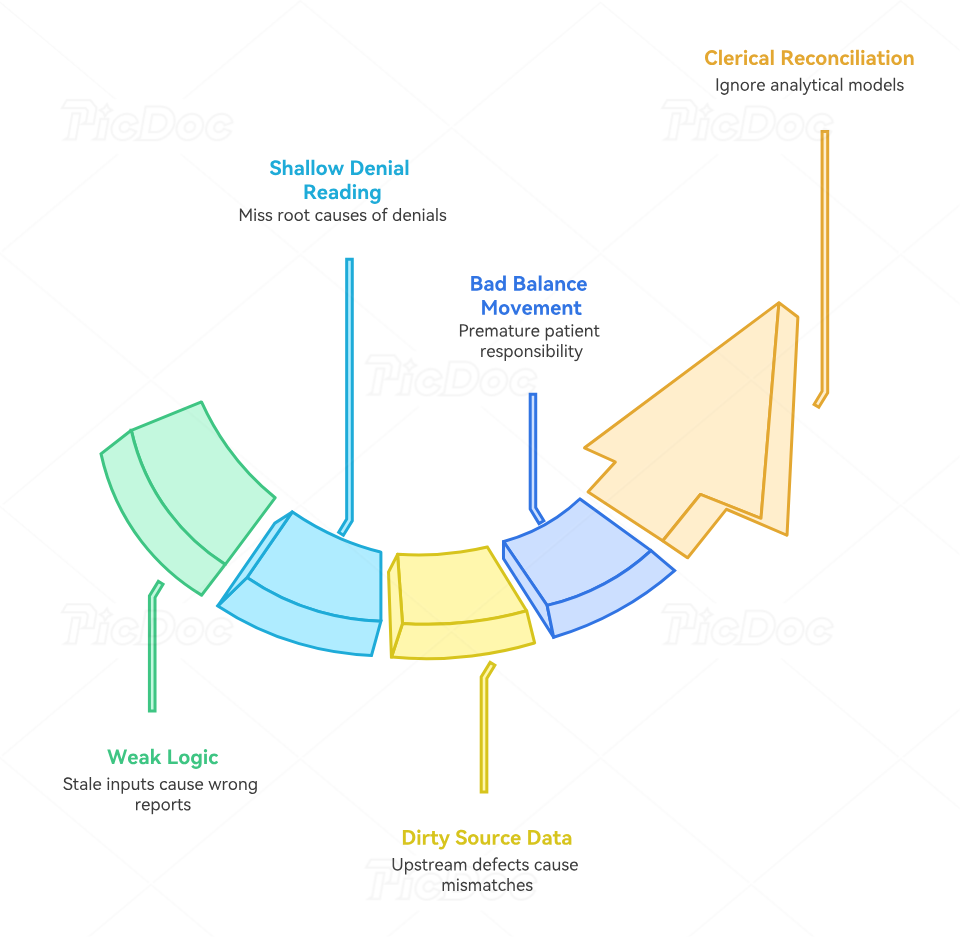
4. The Failure Points That Break Reconciliation and Quietly Drain Revenue
The first major failure point is weak expected-payment logic. Teams cannot identify underpayments if they do not know what should have been paid. That logic depends on fee schedule terminology, Medicare reimbursement rules, commercial insurance billing terms, telemedicine billing guidance, and reimbursement model forecasts. If those inputs are stale, your reconciliation report can look polished while being mathematically wrong.
The second failure point is shallow denial reading. A denial is not a category; it is a story. Staff who read only the headline denial reason miss the operational root cause buried in CARCs, RARCs, EOB narratives, coding edits and modifiers, and denials management analysis. That is how the same denial repeats for months under slightly different code combinations.
The third failure point is dirty source data. Reconciliation gets blamed for upstream defects it did not create. Missing provider identifiers, broken plan selection, incomplete authorizations, incorrect modifier logic, poor EHR documentation habits, unstable problem lists, weak query process standards, and poor documentation accuracy practices all create downstream mismatches. Reconciliation teams need permission to escalate upstream defects rather than merely clean up after them.
The fourth failure point is bad balance movement. Patient responsibility often gets pushed prematurely because staff trust payer output without validating COB sequencing, copay and deductible terminology, medical necessity support, HIPAA and compliance requirements, and billing compliance penalties. Once a bad balance reaches the patient statement cycle, the cost of correction rises sharply.
The fifth failure point is treating reconciliation as clerical instead of analytical. Modern reimbursement is affected by more than a simple fee schedule. Value-based care terms, MACRA terminology, MIPS concepts, ACO billing terms, and risk adjustment coding all influence whether the organization is interpreting payment performance correctly. Reconciliation teams that ignore these models can close accounts while still missing broader reimbursement erosion.
5. Best Practices for Building a Reconciliation Process That Actually Holds Up
First, define one source of truth for expected reimbursement. That source should combine payer contracts, fee schedule rules, modifier logic, site-of-service rules, and known coverage edits. Support it with RCM software terminology, practice management system controls, coding automation terminology, future billing software innovation trends, and predictive analytics in medical billing. Without a trusted expected-payment engine, underpayment detection remains mostly anecdotal.
Second, assign every variance category to a named owner. Reconciliation fails when every exception lands in one generic follow-up queue. Build separate ownership for registration defects, coding defects, documentation defects, payer underpayments, appealable denials, unapplied cash, credit balances, and refund actions using coding workflow terminology, clinical documentation integrity, medical coding audits, denials prevention, and revenue leakage prevention. Ownership transforms analysis into cash.
Third, measure the right KPIs. At minimum, track encounter-to-charge lag, charge-to-claim lag, clean claim rate, rejection rate, initial denial rate, posting lag, underpayment rate, unapplied cash aging, credit balance aging, zero-balance accuracy, and recovery yield on payer variances. Those measures become more meaningful when tied to revenue cycle KPIs, coding productivity benchmarks, coding error reports, RCM efficiency benchmarks, and hospital reimbursement analyses.
Fourth, perform reconciliation in layers and on a schedule. Daily work should cover missing charges, rejected claims, unposted remits, and unapplied cash. Weekly work should cover high-dollar variances, repeated CARC/RARC patterns, rebills, and payer trend shifts. Monthly work should cover refunds, credit balances, bank reconciliation, and close-quality review using payment posting guidance, medical billing RCM mastery, claims adjustment code analysis, billing compliance trends, and medical coding audit terms. Good timing reduces backlog before backlog becomes blindness.
Fifth, treat reconciliation as a learning engine. Repeated mismatches should improve templates, edits, training, and documentation standards. Use trends from coding education and training terms, essential study strategies for coding students, medical billing exam terminology, credentialing organizations, and continuing education for coders. Reconciliation is not only about closing accounts correctly. It is about making tomorrow’s accounts cleaner than today’s.
6. FAQs About Medical Billing Reconciliation Terms
-
Payment posting records what the payer or patient paid. Reconciliation tests whether the posting was correct in light of EOB detail, CARCs, RARCs, expected reimbursement rules, and RCM KPIs. Posting is transactional. Reconciliation is analytical and corrective.
-
The most important terms are allowed amount, contractual adjustment, expected reimbursement, variance, payer takeback, and recoupment. To use them correctly, teams usually need fluency in fee schedule terminology, Medicare reimbursement, commercial payer billing terms, revenue leakage prevention, and impact of coding accuracy on revenue.
-
Because both stop cash, but they stop it at different stages. Rejections happen before adjudication, while denials happen during adjudication. That distinction is built into clearinghouse terminology, medical claims submission workflow, denials management guidance, coding workflow terms, and billing software controls. If you age them together, performance data becomes misleading.
-
Coordination of benefits determines which payer should pay first and what liability should move next. If COB is wrong, primary denials, secondary claim errors, and bad patient balances follow. That is why COB must be checked alongside patient responsibility terms, EOB review, ethical billing principles, and HIPAA compliance changes.
-
It should verify that the claim was accepted, adjudicated correctly, posted correctly, matched to deposits, cleared of unapplied cash, free of unresolved credit balances, and billed correctly to the patient when appropriate. That review should lean on payment posting management, coding audits, medical record retention requirements, billing compliance trend analysis, and revenue leakage prevention.
-
Do three things immediately: build expected-payment logic, map top variance types to owners, and measure posting lag plus unapplied cash daily. Those actions become far stronger when supported by RCM terms, revenue cycle benchmarks, coding productivity benchmarks, automation terms, and future billing software innovation. Fast improvement comes from visibility, ownership, and timing—not from more manual effort alone.