
Directory of Medicare Billing Tools & Resources
Medicare billing falls apart when teams rely on memory instead of tools. Claims get delayed because eligibility was not verified, documentation did not support medical necessity, modifiers were applied loosely, remittance codes were misread, and staff could not trace where the breakdown actually began. That is why a real Medicare billing directory matters.
This guide gives coders, billers, auditors, office managers, and revenue cycle leaders a practical map of the tools and resources that keep Medicare billing accurate, faster, and easier to defend. Use it to reduce denials, tighten workflows, and strengthen reimbursement across the full claim life cycle.
1. Why Medicare Billing Tools Matter More Than Most Teams Think
Many teams treat Medicare billing as if it is just another payer workflow with slightly stricter rules. That mindset creates avoidable damage. Medicare claims are deeply tied to documentation support, coverage rules, frequency limits, status logic, place-of-service accuracy, modifier discipline, and remittance interpretation. One weak step upstream can turn into downstream losses in payment posting, claims reconciliation, medical billing reconciliation, and revenue leakage prevention.
The strongest Medicare billing teams do not depend on one “expert” who knows everything. They build a repeatable tool stack. That stack includes eligibility checks, fee schedule references, coding standards, modifier guidance, remittance code references, documentation requirement checklists, clearinghouse edits, denial analysis tools, audit workpapers, and reporting dashboards. When staff know where to look, they stop guessing. That discipline aligns naturally with stronger use of revenue cycle management terms, healthcare claims management terms, clearinghouse terminology, and EDI billing terms.
The pain point is rarely the claim form by itself. The real pain point is fragmented workflow. One team verifies eligibility in one system, another enters codes in a separate system, someone else posts payments from a remittance screen they only half understand, and nobody owns the denial root cause. Medicare punishes disconnected workflow. A strong resource directory brings those moving parts together and supports better performance in CMS-1500 form usage, UB-04 form logic, accurate reimbursement practices, and revenue cycle KPIs.
Another reason tools matter is speed under pressure. Medicare billing teams handle repeated questions that sound small but carry major consequences. Was the patient eligible on the date of service? Does this service meet frequency limits? Which modifier is appropriate? Is the denial tied to missing documentation, duplicate billing, bundling, or medical necessity? How should the team interpret the remittance? What should be appealed and what should be corrected? When these questions get answered late, cash slows down. When they get answered wrong, denials multiply. Teams that stay sharp usually cross-train around Medicare reimbursement concepts, physician fee schedule terms, patient responsibility terms, and commercial-versus-government billing logic.
Medicare Billing Tools & Resources Map: What Each One Does and Why It Matters (25+ Rows)
| Tool / Resource | What It Helps You Do | Why It Matters in Medicare Billing | Best Practice Action |
|---|---|---|---|
| Eligibility verification tool | Confirms active coverage and payer details | Wrong eligibility leads to rejections before real adjudication begins | Verify on the date of service, not just at scheduling |
| Medicare fee schedule reference | Checks payment rates and status indicators | Prevents incorrect reimbursement expectations | Use it before quoting value or investigating underpayments |
| NCCI edit resource | Flags bundling conflicts between codes | Reduces denials tied to improper unbundling | Review before final claim submission when multiple procedures appear |
| LCD and coverage policy reference | Shows service-specific medical necessity conditions | A service can be coded correctly and still fail coverage | Pair diagnosis review with coverage review |
| Medical necessity checklist | Aligns documentation to billed service | Weak necessity is a major denial driver | Make it specialty-specific where possible |
| Modifier reference guide | Helps apply modifiers accurately | Modifier misuse creates denials and audit exposure | Require documentation support before modifier use |
| CARC lookup tool | Explains claim adjustment reason codes | Without it, denial teams misclassify root causes | Tie every adjustment to a tracked action path |
| RARC lookup tool | Clarifies remittance advice remark codes | Remarks often explain the real operational failure | Read with CARCs, not separately |
| Remittance viewer | Shows payment, adjustment, and remark details | Essential for accurate payment posting | Train staff to trace line-level outcomes |
| Claim scrubber | Catches format and logic errors before submission | Prevents avoidable rejections and edits | Use edit reports as a training source, not just a gate |
| Clearinghouse dashboard | Tracks transmission status and rejection patterns | Shows whether failures happen before payer adjudication | Separate clearinghouse edits from payer denials in reporting |
| Charge capture audit sheet | Verifies services entered match services performed | Missing charges and duplicate charges both hurt revenue | Audit by provider and service type monthly |
| EHR documentation review tool | Checks note support for codes and services | Claims fail when documentation lags behind coding detail | Build specialty-based smart checklists |
| ABN workflow reference | Guides advance beneficiary notice handling | Improper handling causes write-offs and patient disputes | Train front-end and billing staff together |
| Appeal template library | Speeds response to denials and underpayments | Inconsistent appeals waste time and weaken recovery | Create denial-specific templates by reason cluster |
| Coding manual / digital encoder | Supports accurate diagnosis and procedure selection | Weak coding logic poisons the whole claim | Update training whenever code changes occur |
| CMS-1500 reference | Supports professional claim field accuracy | Field-level mistakes cause preventable delays | Map common denial patterns back to form fields |
| UB-04 reference | Supports institutional billing field logic | Critical for facility claims and inpatient/outpatient logic | Review revenue code and bill type training often |
| Coordination of benefits resource | Clarifies primary versus secondary payment order | Wrong sequencing causes rejections and delayed cash | Verify COB before submitting crossover assumptions |
| Patient responsibility estimator | Projects deductible, coinsurance, and related balance exposure | Reduces confusion and collection friction | Use it before service when possible |
| Denial trend dashboard | Groups denials by root cause and impact | Shows where the system is bleeding cash repeatedly | Track by provider, service, and department |
| Aging report | Shows unpaid claim inventory over time | Prevents older Medicare balances from disappearing into backlog | Split by claim status, not just age bucket |
| Audit workpaper template | Standardizes internal billing audits | Finds control failures before external review does | Use sample-based recurring audits, not one-off reviews |
| Provider education tracker | Documents repeated documentation and billing issues by provider | Turns denial data into targeted improvement | Tie training topics to measurable claim outcomes |
| RCM KPI dashboard | Tracks clean claim rate, denial rate, days in AR, and recovery | Without metrics, teams fix noise instead of core problems | Review trends weekly and monthly |
| Coding-compliance checklist | Aligns code choice with documentation and policy | Protects against overcoding and unsupported billing | Build one for each high-risk service line |
| Data export / analytics tool | Turns claim activity into usable reporting | Essential for spotting underpayments and repeat edits | Use line-item detail, not only summary totals |
| Record retention tracker | Maintains access to needed documentation and support files | Weak retention cripples audits and appeals | Align retention with billing and compliance needs |
| Credentialing / enrollment status tracker | Checks whether provider billing setup is active and correct | Enrollment issues can stop payment completely | Audit roster and billing setup regularly |
2. The Core Medicare Billing Tools Every Team Should Actually Use
The first non-negotiable tool is eligibility verification. Medicare billing errors often begin because staff assume coverage is active, primary, and unchanged. That assumption can fail when a patient’s coverage status shifts, a secondary payer is involved, or an administrative detail changed between scheduling and the date of service. Eligibility checks should happen early, but strong teams verify again when it matters. This reduces false starts across coordination of benefits workflows, patient responsibility review, healthcare billing acronyms, and practice management systems.
The second essential category is pricing and payment logic resources. Teams need fast access to fee schedule information, coverage rules, and service status logic. Without that, staff cannot tell whether a payment shortfall is real, whether a service was billed in the right setting, or whether the claim even had a path to payment under Medicare rules. This is where physician fee schedule terms, Medicare reimbursement references, value-based care terms, and cost reporting concepts become operationally useful instead of theoretical.
Third, teams need coding and edit-control tools. A claim can fail even when the diagnosis and procedure seem individually correct. Medicare logic also cares about bundling, modifier support, diagnosis-to-service linkage, and field-level consistency. That is why strong departments rely on coding edits and modifiers guidance, CPT modifier explanations, medical coding workflow references, and medical necessity criteria before the claim ever leaves the system.
Fourth, remittance and denial tools matter just as much as front-end tools. Many organizations work hard to get claims out the door but stay weak at understanding how Medicare paid them back. That is where money quietly disappears. If your team cannot read adjustment and remark codes fluently, it cannot separate write-off logic from fixable underpayments, or payer policy from internal workflow failure. That is why every Medicare billing resource directory should heavily emphasize CARC references, RARC dictionaries, EOB understanding, and collections and bad debt prevention.
Finally, reporting and audit tools transform one-off fixes into system improvement. Teams that do not track clean claim rate, denial clusters, days in AR, and recovery outcomes end up reacting emotionally instead of operationally. Medicare billing becomes easier when the department can prove where it is losing time, cash, and accuracy.
3. How to Use Medicare Resources to Prevent Denials Instead of Just Responding to Them
The most expensive Medicare billing teams are not the ones with the most denials. They are the ones with the most repeated denials. Repetition means the organization is learning too slowly. Tools and resources should be structured to stop recurrence, not simply help staff survive it. That requires a prevention sequence: verify eligibility, validate documentation, review coding logic, check edit conflicts, submit cleanly, interpret remittance correctly, and feed patterns back into training. This same discipline supports stronger outcomes in coding audit work, coding ethics and standards, medical coding regulatory compliance, and medical record retention.
Start with service-level necessity, not claim-level cleanup. Medicare often denies claims that look technically correct because the documentation never justified the service in the first place. A medical necessity checklist built by specialty is one of the highest-return resources a billing department can create. For cardiology, that might mean ensuring symptom severity, test rationale, and follow-up indication are clear. For therapy, it may mean function-based support. For injections, it may mean diagnosis linkage and administration detail. Teams that standardize necessity review do better in infusion and injection billing, ambulance and emergency transport coding, lab and pathology coding, and telemedicine coding.
Next, use remittance codes as process intelligence. Too many teams post the payment, note the denial, and move on. A better system translates each CARC and RARC combination into an operational cause. Was registration wrong? Was coding under-supported? Was a modifier misused? Was the service noncovered? Was documentation missing? Was it duplicate billing? Was it a timing issue? When teams map codes to action categories, denial management becomes measurable instead of chaotic.
Then create appeal resources that are selective and disciplined. Not every Medicare denial deserves the same energy. Some should be corrected and rebilled. Some need documentation. Some need policy-based appeal language. Some represent true nonpayment. A good appeal template library helps staff move faster without becoming careless. The point is not to send more appeals. The point is to send smarter appeals.
Quick Poll: What is your biggest Medicare billing pain right now?
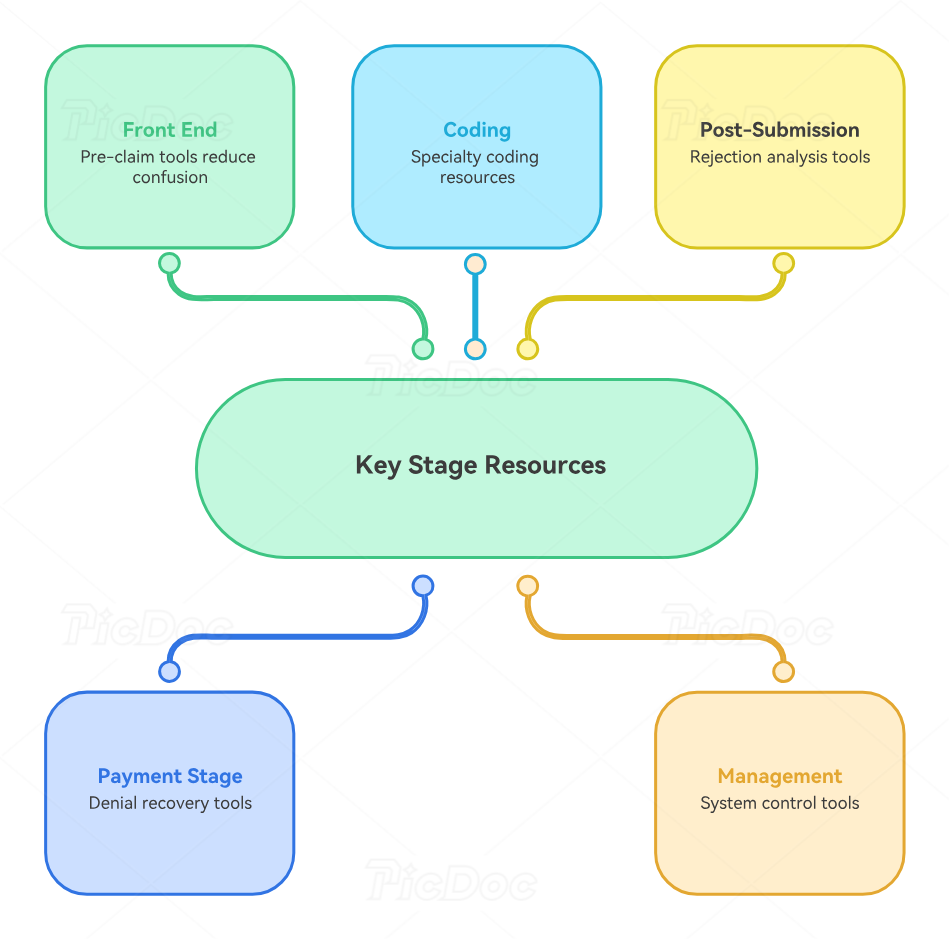
4. The Most Valuable Medicare Billing Resources by Workflow Stage
At the front end, the best resources are eligibility tools, Medicare payer sequencing references, ABN workflows, and patient responsibility estimators. These reduce avoidable confusion before the claim even exists. Front-end failure creates expensive back-end labor, so this stage deserves more respect than it usually gets. Teams that strengthen intake usually see benefits later in charge capture accuracy, encounter form use, EHR documentation terms, and EMR documentation workflow.
During coding and claim creation, the highest-value resources are fee schedule references, diagnosis and procedure coding tools, modifier guides, bundling edit tools, specialty-specific billing references, and specialty documentation checklists. Different departments need different supporting resources. Emergency medicine teams benefit from CPT codes for emergency medicine. Cardiology teams need cardiology procedure coding guidance. Radiology teams need radiology coding references and radiology billing dictionaries. Specialty tools shorten lookup time and improve confidence.
After submission, clearinghouse dashboards and rejection reports become critical. Teams must separate technical rejection from payer adjudication failure. These are different problems and should never be blended in reporting. When they are blended, management misreads the real failure pattern and trains the wrong people.
At the payment and denial stage, remittance viewers, CARC and RARC references, denial work queues, aging reports, and appeal template libraries carry the most value. This is where operational intelligence is either captured or wasted. The organizations that recover more Medicare cash are usually the ones that document denial patterns best, not the ones that simply work hardest.
At the management layer, KPI dashboards, audit templates, training trackers, and data export tools are what turn Medicare billing from a reactive function into a controllable system. Without these, teams live in a constant state of firefighting.
5. How to Build a Medicare Billing Resource System Your Team Will Actually Use
The best directory is the one staff can use in under thirty seconds. Most billing departments already have resources scattered across email threads, shared drives, tribal memory, PDF folders, and payer portals. That is not a usable system. A real Medicare billing resource system should be organized by workflow stage, not by whoever uploaded the file last. Front end, coding, claim submission, remittance, denial, appeals, and audit should each have their own tool cluster.
Each resource should answer one primary question. Eligibility tool: is coverage active and primary? Fee schedule: what should this service pay and under what status logic? Modifier guide: when is this modifier defensible? CARC/RARC reference: why did payment change? Appeal template: what response path fits this denial? Audit sheet: what control failed? When tools are too broad, staff stop trusting them.
The next step is ownership. Every major Medicare resource should have an owner responsible for updates, training impact, and usage quality. If nobody owns the modifier guide, it goes stale. If nobody owns the denial dashboard, it becomes decorative. If nobody owns appeal templates, staff improvise weak responses. Resource ownership is not bureaucracy. It is protection against decay.
Then embed the resource system into training. New staff should learn the directory during onboarding, and experienced staff should see how the same resources support different specialties and denial types. Use real cases. Show how an eligibility miss became a denial, how a modifier misstep triggered rework, how a remittance clue exposed a deeper workflow failure. Adults learn Medicare billing faster when training is tied to money and consequences, not abstract definitions alone.
Finally, keep the directory tied to results. If a resource exists but does not improve clean claim rate, denial rate, appeal success, turnaround time, or underpayment recovery, refine it. Medicare billing tools are useful only when they change outcomes.
6. FAQs
-
For many small teams, the most important starting tool is a combined eligibility and remittance discipline. Eligibility prevents false starts, and remittance understanding prevents silent losses after payment. Small teams often focus heavily on claim submission while underinvesting in what happens before and after the claim. That creates avoidable denials and missed recovery opportunities.
-
They repeat because the organization is treating denials as tasks instead of signals. A denial should point back to a broken rule, weak process, documentation gap, or training issue. Without a dashboard that groups denials by root cause, staff keep fixing symptoms while the system keeps producing the same damage.
-
The most helpful resources are a clear modifier reference, an edit-check tool, service-specific documentation checklists, and denial trend reporting. Modifier errors rarely come from ignorance alone. They usually come from unsupported use, rushed use, or failure to understand how the billed services interact. Teams need tools that connect modifier logic to documentation and edits, not just a static list of definitions.
-
Start with the denial reason and the operational cause. If the issue is a fixable claim error, correction and resubmission may be the right path. If the claim was denied despite correct billing and sufficient support, an appeal may be appropriate. The decision gets easier when the team uses CARCs, RARCs, documentation review, and policy references together instead of in isolation.
-
A useful dashboard shows clean claim rate, rejection rate, denial rate, top denial reasons, appeal recovery, days in AR, underpayment patterns, and performance by provider or service line. It should separate front-end errors, clearinghouse issues, payer denials, and posting outcomes. A dashboard that only reports totals hides the real leak points.
-
Teach the tools in claim order. Start with eligibility and patient setup, then coding support, then claim form logic, then edits, then remittance reading, then denial recovery, then reporting. Pair each tool with one real billing question it solves. That approach builds operational confidence much faster than handing new staff a giant library and expecting them to memorize it.