
ICD-11 Reference Directory for Oncology
Oncology coding breaks down fast when coders rely on broad disease labels, partial pathology language, or incomplete treatment context. Cancer claims are rarely simple. The chart may contain primary malignancy details, histology clues, staging references, treatment complications, secondary spread, follow-up status, and symptom documentation that all affect code selection, sequencing logic, and reimbursement integrity.
This reference directory is built to solve that problem. It organizes high-value ICD-11 oncology terms into a practical coding guide that helps you read cancer documentation more precisely, avoid claim-level mistakes, support medical necessity, and work more confidently across diagnosis, treatment, recurrence, and long-term oncology follow-up.
1. Why oncology coding in ICD-11 demands sharper documentation reading
Oncology coding punishes guesswork more aggressively than many other specialties because cancer documentation is layered, longitudinal, and often written by multiple clinicians across surgery, pathology, medical oncology, radiation oncology, and follow-up care. A coder may see “breast cancer,” “mass,” “history of malignancy,” “metastatic disease,” and “currently on immunotherapy” in the same chart and still need to determine what is active, what is historical, what is suspected, and what is merely part of the differential. That is why anyone working through oncology records should ground themselves in ICD-11 coding standards and best practices, ICD-11 mental health coding dictionary clear definitions and examples, ICD-11 codes for neurological disorders essential reference, and ICD-11 coding essentials for respiratory diseases explained so the logic of ICD-11 specificity becomes second nature across specialties.
Cancer records also expose a common coding weakness: confusing clinical momentum with coded certainty. A patient may be receiving workup for a suspicious lesion, but suspicion is not confirmation. A pathology result may later confirm invasive disease, but the coder still needs to align the timing of that confirmation to the encounter being coded. This is where the discipline taught in medical necessity criteria essential coding guide, clinical documentation improvement CDI terms dictionary, complete reference for coding query process terms, and guide to electronic medical records EMR documentation terms becomes essential. Strong oncology coders do not chase dramatic terms. They trace support.
Another reason oncology coding is difficult is that diagnosis selection often intersects with treatment phase. A cancer chart may reflect newly diagnosed disease, neoadjuvant treatment, post-operative pathology reconciliation, recurrence assessment, palliative symptom management, or surveillance after remission. Each scenario changes what matters most in the note. Coders who treat every oncology record as “site plus malignancy” miss the clinical frame that shapes reimbursement and compliance. That is why oncology work benefits from the broader operational thinking found in medical coding workflow terms complete reference, guide to accurate medical billing and reimbursement, medical coding audit terms comprehensive dictionary, and guide to medical coding regulatory compliance.
The bottom line is simple: oncology coding is not hard because cancer is complex in the abstract. It is hard because small documentation misreads can distort disease status, staging context, treatment justification, and downstream claims integrity. ICD-11 rewards precision, and oncology exposes every place where a coder’s precision is weak.
| Term | What It Means | Why It Matters in Oncology Coding | Best Practice Action |
|---|---|---|---|
| Primary malignancy | Original site where the cancer started | Drives code assignment, sequencing, and treatment context | Confirm site from definitive documentation, not assumptions |
| Secondary malignancy | Metastatic spread to another site | Often changes clinical picture and claim logic | Code documented metastatic sites separately when supported |
| Histology | Microscopic tumor cell type | Can affect cancer specificity and treatment interpretation | Use pathology-confirmed language when available |
| Neoplasm behavior | Benign, in situ, uncertain, or malignant character | Wrong behavior selection distorts severity and billing | Do not upcode uncertain terms into confirmed malignancy |
| In situ | Localized abnormal cells without invasion | Different from invasive cancer and must stay distinct | Check pathology wording carefully before assigning invasive disease |
| Remission | Reduction or disappearance of cancer signs | Affects active treatment versus surveillance coding context | Code current documented status, not old disease activity |
| Recurrence | Return of cancer after prior response or remission | Changes medical necessity and oncology follow-up logic | Look for explicit provider language showing return of disease |
| Residual disease | Cancer remaining after treatment | Important in post-treatment coding and clinical interpretation | Differentiate residual disease from treatment effect |
| Metastasis | Spread of malignant cells from primary site | High-impact coding detail for oncology claims | Capture supported metastatic sites with precision |
| Staging | Extent of disease spread and severity | Supports treatment intensity and risk interpretation | Do not convert vague stage references into unsupported specifics |
| TNM | Tumor, node, metastasis staging framework | Common oncology documentation language | Use as context when explicitly documented by clinician |
| Tumor marker | Biologic indicator associated with malignancy | Supports workup and follow-up context, not diagnosis alone | Avoid coding cancer from marker results alone |
| Biopsy-proven | Diagnosis confirmed by tissue examination | Strengthens diagnostic certainty | Prioritize definitive pathology-supported documentation |
| Suspected malignancy | Cancer not yet confirmed | Common trap in oncology workups | Code symptoms and findings unless malignancy is confirmed |
| Oncology surveillance | Monitoring after treatment for recurrence or progression | Affects visit purpose and diagnosis context | Read encounter reason, not just cancer history |
| Active treatment | Current therapy directed at malignancy | Separates ongoing management from historical status | Link encounter diagnosis to treatment phase |
| Adjuvant therapy | Treatment after primary therapy to reduce recurrence | Shapes oncology treatment coding context | Differentiate adjuvant from palliative or neoadjuvant intent |
| Neoadjuvant therapy | Treatment before primary procedure | Frequently appears in surgical oncology records | Confirm treatment timing in relation to surgery |
| Palliative treatment | Therapy aimed at symptom control rather than cure | Important for severity and care-plan interpretation | Use documented care intent, not assumption from disease stage |
| Complication of treatment | Adverse effect from cancer therapy | Can drive separate coding and reimbursement issues | Identify relationship between therapy and documented complication |
| Anemia due to malignancy | Anemia linked to cancer burden | Etiology affects coding choice and sequencing logic | Use provider-documented cause, not inference |
| Neutropenia | Low neutrophil count, often treatment related | Common oncology admission driver | Distinguish disease-related from chemotherapy-induced when documented |
| Cachexia | Cancer-associated wasting syndrome | Impacts acuity and supportive care picture | Capture only when clearly documented and clinically supported |
| Pathology report | Definitive tissue-based findings | Central to accurate oncology specificity | Reconcile pathology with progress notes and operative reports |
| Molecular finding | Genetic or biomarker characteristic of tumor | Increasingly important in oncology documentation | Use only if coding rules and documentation support it |
| History of malignancy | Past cancer no longer under active management | A frequent source of overcoding active cancer | Separate personal history from active disease carefully |
| Cancer-related symptom | Pain, weight loss, fatigue, obstruction, bleeding, etc. | May affect encounter focus and medical necessity | Check whether symptom is integral, associated, or separately managed |
2. Core ICD-11 oncology directory terms coders must master first
The first cluster of terms you must control includes primary malignancy, secondary malignancy, metastasis, in situ disease, recurrence, remission, residual disease, and history of malignancy. These are not interchangeable labels. They represent materially different clinical realities that affect code assignment, sequencing, medical necessity, and even payer interpretation. The fastest way to create oncology claim risk is to collapse those distinctions into one vague cancer label. For that reason, coders should regularly reinforce their foundation with ICD-11 oncology codes detailed dictionary and case studies, ICD-11 coding standards and best practices, guide to health information management HIM terms, and electronic health record EHR coding terms dictionary.
Primary versus secondary malignancy is one of the most important distinctions in oncology documentation. The primary site identifies where the cancer originated. Secondary sites reflect metastatic spread. That sounds easy until you open real charts filled with shorthand language, copied forward notes, partial pathology references, and specialist-specific vocabulary. A progress note may mention “mets to liver” while another section focuses on “colon cancer on chemotherapy,” and the coder must determine what is active, what is supported, and how the note frames the current encounter. Skills from comprehensive guide to SOAP notes and coding, comprehensive guide to problem lists in medical documentation, medicare documentation requirements for coders, and medical record retention and storage terms help you verify which source carries the strongest support.
Histology, behavior, and pathology language form the second foundational layer. In oncology, site alone often fails to tell the whole story. Histologic type, behavior status, and biopsy confirmation can shape specificity and interpretation. A coder who ignores pathology detail may undercode, overstate disease certainty, or miss the line between uncertain neoplasm language and confirmed malignancy. That is why coders benefit from the precision mindset found in guide to lab and pathology coding essentials, medical abbreviations and acronyms dictionary for coders, healthcare billing acronyms comprehensive dictionary and examples, and guide to clinical decision support CDS terms for coders, because oncology charts often use compact language that carries large coding consequences.
Finally, coders must understand that “history of malignancy” is not a safe placeholder when the chart actually supports active disease, and “active cancer” is not a safe assumption when the note documents surveillance after completed treatment. That distinction affects reimbursement, utilization review, quality reporting, and audit defensibility. It is one of the most expensive errors in outpatient oncology coding because it looks subtle yet can materially alter the meaning of the claim.
3. Treatment-phase, complication, and sequencing terms that create the biggest oncology coding mistakes
The next layer of oncology terminology revolves around treatment intent and disease phase. Coders need to separate active treatment, neoadjuvant therapy, adjuvant therapy, palliative therapy, surveillance, remission, recurrence assessment, and treatment complication management. When these terms are misunderstood, coders often misread the purpose of the encounter. A patient may come in for management of chemotherapy-related neutropenia, post-radiation complications, or surveillance imaging after remission, and those scenarios are not interchangeable. This is where infusion and injection therapy billing terms explained, reference anesthesia coding and billing terms, telemedicine coding terms and definitions explained, and hospice and palliative care coding detailed dictionary help coders understand how treatment context shapes the entire encounter.
Complications are another major trap. Oncology records frequently include anemia, neutropenia, dehydration, nausea, pain crises, infection risk, cachexia, treatment intolerance, and organ-specific side effects. A coder has to determine whether the condition is documented as caused by the malignancy itself, the therapy, another comorbidity, or a still-undetermined process. Guessing causality creates claim risk fast. You need the same disciplined approach used in guide to utilization review and management terms for coders, guide to healthcare claims management terms, guide to claim adjustment reason codes CARCs, and remittance advice remark codes RARCs comprehensive dictionary, because unclear causation often becomes denial-causing ambiguity later.
Sequencing logic in oncology also requires maturity. Sometimes the malignancy drives the encounter. Sometimes the symptom, treatment adverse effect, follow-up status, or supportive management issue frames the medical necessity of the visit. Strong coders do not force a fixed sequencing pattern onto every oncology record. They look at why the patient is being seen today, what condition is being evaluated or managed, how the provider defines the problem, and what documentation supports that focus. That approach is strengthened by studying guide to physician fee schedule terms, commercial insurance billing terms essential guide, guide to payment posting in medical billing, and medical billing reconciliation terms comprehensive guide, because payers scrutinize encounter logic through the claim outcome, not through coder intentions.
Many oncology coding failures happen because coders read cancer charts like static snapshots. Oncology documentation is longitudinal. You must see where the patient is in the disease journey and code the encounter in that context. Without that habit, copied-forward language, outdated problem lists, and old disease labels will pull your coding in the wrong direction.
4. How oncology documentation should be read before you ever assign an ICD-11 code
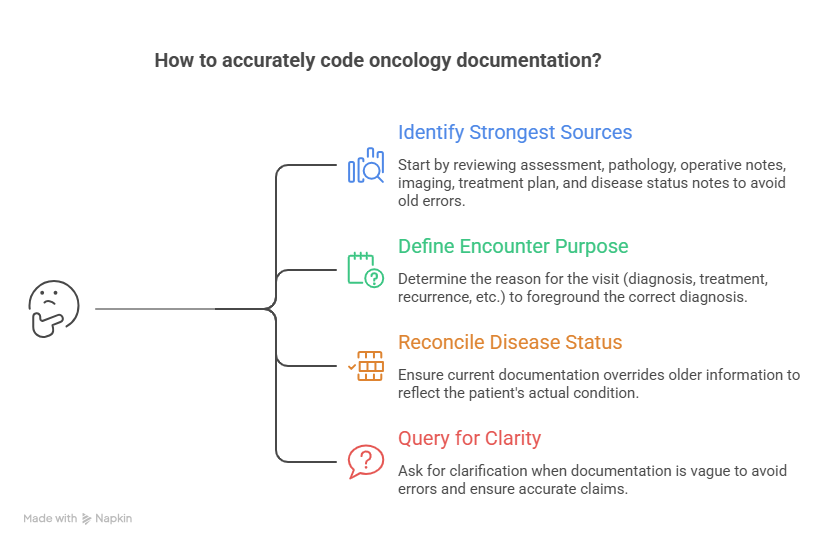
The best oncology coders do not start with the diagnosis line. They start by identifying the strongest documentation sources in the chart. In cancer records, that usually means reviewing the assessment and plan, pathology report, operative note if relevant, imaging impression when clinically tied to the encounter, current treatment plan, and any note that clearly states disease status. Coders who jump straight to the problem list or copied diagnosis header often inherit old errors. That is why reading discipline from guide to electronic medical records EMR documentation terms, electronic health record EHR coding terms dictionary, complete reference for encoder software terms, and guide to revenue cycle management software terms is crucial in oncology.
Next, define the encounter purpose. Is the patient being seen for diagnosis confirmation, active treatment, treatment planning, recurrence evaluation, surveillance after prior therapy, or management of a complication? That purpose often decides which diagnosis should be foregrounded and which documented conditions are contextual. A coder who misses encounter purpose may technically capture disease terms yet still produce a claim that feels clinically incoherent. Practical framing skills from guide to accurate medical billing and reimbursement, guide to healthcare claims management terms, revenue cycle management RCM terms explained, and revenue cycle metrics and KPIs terms and definitions help coders align coding logic with how claims are actually judged.
Then reconcile disease status across the note. If the oncologist documents “metastatic breast cancer with liver involvement on maintenance therapy,” but the problem list still says “history of breast cancer,” the coder should not let the problem list override the current assessment. If pathology supports invasive adenocarcinoma but the older imaging note used “suspicious mass,” current definitive documentation governs. That habit reflects the exact mindset developed through medical coding audit terms comprehensive dictionary, complete guide to coding ethics and standards, guide to medical coding regulatory compliance, and healthcare data security terms for medical coders, because disciplined chart interpretation is both a quality and compliance issue.
Finally, look for what the chart does not quite say. Oncology records often need queries when provider language does not clearly distinguish primary versus metastatic disease, treatment-related versus disease-related complications, current activity versus historical status, or the reason the patient is being seen today. Querying is not a sign of weakness. In oncology, it is often what keeps a coder from locking vague or contradictory language into a billable claim.
5. How this ICD-11 oncology directory improves claim quality, compliance, and coder confidence
A strong oncology directory is not just a glossary. It is a decision support tool. Its value comes from helping coders connect cancer language to documentation support, encounter purpose, sequencing logic, and downstream payment integrity. When coders internalize oncology terms this way, they reduce vague code selection, strengthen medical necessity alignment, and make it easier for auditors, billers, and revenue-cycle teams to follow the logic of the claim. That broader payoff is why oncology coders should also work through guide to medical coding revenue leakage prevention, comprehensive guide to charge capture terms, advanced guide to claims reconciliation terms, and understanding collections and bad debt in medical billing, because oncology miscoding often becomes hidden revenue loss long before it becomes a visible audit issue.
This kind of directory also builds speed without sacrificing safety. Many coders slow down in oncology because every chart feels unstable. That usually happens when terminology is only half understood. Once you can quickly separate biopsy-confirmed disease from suspected disease, active treatment from surveillance, metastasis from primary site, and treatment complication from unrelated condition, your review becomes more systematic. Resources like understanding coding edits modifiers complete guide, CPT modifiers dictionary usage and examples explained, understanding medical coding system updates and releases, and guide to data analytics and reporting terms for coders help coders turn that systematic thinking into measurable performance.
It also prepares coders for the growing complexity of oncology data environments. Modern oncology care increasingly blends diagnosis coding, treatment documentation, pathology detail, biomarker discussion, risk adjustment implications, and longitudinal follow-up across settings. Coders who can navigate that ecosystem are more future-proof than coders who depend on memorized site lists. That is why it helps to build related fluency through hierarchical condition categories HCCs coding definitions, value-based care coding terms explained, Medicare Access and CHIP Reauthorization Act MACRA terms, and comprehensive guide to risk adjustment coding. Even when those frameworks do not directly decide the oncology diagnosis code, they shape how coded data is used beyond the claim itself.
Most importantly, a high-quality oncology reference directory creates confidence rooted in process rather than guesswork. That is the kind of confidence that survives audits, denials, and complex chart reviews. It is not loud confidence. It is defensible confidence.
6. FAQs
-
Oncology coding demands sharper distinction between confirmed disease, suspected disease, active malignancy, historical malignancy, recurrence, remission, metastatic spread, and treatment complications. Cancer charts are also highly longitudinal, so old language can easily contaminate current coding logic. Coders need the same disciplined approach promoted in ICD-11 coding standards and best practices, clinical documentation improvement CDI terms dictionary, guide to electronic medical records EMR documentation terms, and medical coding audit terms comprehensive dictionary.
-
Read the current assessment and plan, treatment section, pathology context, and encounter purpose before trusting the problem list. Active treatment, surveillance, recurrence evaluation, and historical status each create different coding implications. This is where comprehensive guide to problem lists in medical documentation, electronic health record EHR coding terms dictionary, medicare documentation requirements for coders, and guide to accurate medical billing and reimbursement help coders verify current status safely.
-
Only when the documentation supports it at the level required for coding. Imaging impressions, oncology assessment language, pathology support, and definitive provider statements all matter. Suggestive wording alone can be dangerous if it has not been clinically confirmed in a codable way. Build that judgment through guide to lab and pathology coding essentials, complete reference for coding query process terms, guide to medical coding regulatory compliance, and complete guide to coding ethics and standards.
-
First determine whether the provider links the complication to the malignancy itself, to therapy, or to another process. Then identify the reason for the encounter and the clinical management focus. Treatment complications can materially change sequencing and reimbursement logic. This becomes easier when you understand infusion and injection therapy billing terms explained, guide to healthcare claims management terms, guide to claim adjustment reason codes CARCs, and remittance advice remark codes RARCs comprehensive dictionary.
-
Because code books and software do not automatically fix weak interpretation. A reference directory organizes the language patterns, chart clues, and decision points that determine whether your coding logic is actually defensible. It works best alongside complete reference for encoder software terms, guide to revenue cycle management software terms, medical coding workflow terms complete reference, and guide to data analytics and reporting terms for coders, because oncology accuracy depends on process more than lookup speed.
-
Stop trying to memorize oncology as a giant disease list. Instead, train yourself to answer the same questions on every chart: what is confirmed, what is active, what is historical, what is the encounter purpose, what is the treatment phase, what complications are documented, and what support is strongest in the record. Pair that habit with repeated review of ICD-11 oncology codes detailed dictionary and case studies, ICD-11 coding standards and best practices, guide to health information management HIM terms, and guide to medical coding revenue leakage prevention. That is how confidence becomes reliable rather than fragile.