
Comprehensive Directory of Claim Adjustment Reason Codes (CARCs)
Claim Adjustment Reason Codes are the difference between “the payer reduced the claim” and “we know exactly why the payer reduced the claim, who owns the fix, and whether money is still recoverable.” CARCs sit inside payment posting, claims reconciliation, denial management, and revenue leakage prevention. When teams misread them, deductible balances get posted incorrectly, denials are appealed with the wrong evidence, underpayments are written off too fast, and repeat errors keep hitting the same payer, provider, code, or location.
1. What CARCs Actually Explain on a Remittance Advice
A CARC explains why a claim or service line was paid differently than it was billed. X12 lists Claim Adjustment Reason Codes as external code list 139 and describes them as codes used when a claim or service line was paid differently from the billed amount; the X12 external code list page shows the CARC list as maintained by CMG03 and last modified on 11/01/2025. For medical billers, that definition matters because the code is not just a denial label. It is the payer’s structured explanation for an adjustment, and it should connect directly to CARC definitions, RARC explanations, EOB interpretation, and healthcare claims management.
The biggest mistake is treating every CARC like a denial. Some CARCs show patient responsibility, such as deductible, coinsurance, or copayment. Some show contractual adjustment. Some show missing information, authorization failure, duplicate billing, non-covered services, bundling, medical necessity, timely filing, coordination of benefits, or payer routing problems. CMS explains that group codes, CARCs, and RARCs are used to explain adjustments at the claim or service-line level, and group codes identify the broad category of the payment adjustment. This is why a strong posting team checks the CARC, group code, payer contract, and remark code before deciding whether the balance belongs to the patient, the provider write-off bucket, the appeal queue, or the correction queue.
CARCs also become powerful when they are grouped by root cause. CARC 16-type issues usually point toward missing or incomplete information. CARC 18-type issues usually point toward duplicate claim behavior. CARC 22-type issues usually point toward coordination of benefits. CARC 29-type issues point toward timely filing. CARC 45-type issues require fee schedule or contract review through accurate reimbursement, physician fee schedule reimbursement, Medicaid reimbursement, and payment posting controls. The code is the start of the investigation, not the whole answer.
| CARC | Plain-English Meaning | What Usually Went Wrong | Best Billing Action |
|---|---|---|---|
| 1 | Deductible-related adjustment | The payer assigned part of the allowed amount to the patient’s deductible. | Post as patient responsibility only after checking patient responsibility terms and plan benefits. |
| 2 | Coinsurance-related adjustment | The payer left a percentage share for the patient or secondary payer. | Validate secondary billing through COB definitions. |
| 3 | Copayment-related adjustment | The claim processed with a fixed patient copay amount. | Confirm benefit rules before moving the balance to collections or bad debt. |
| 4 | Procedure and modifier conflict | The submitted CPT/HCPCS code and modifier combination does not fit payer rules. | Review CPT modifier guidance before correcting. |
| 5 | Procedure, bill type, or place-of-service mismatch | The service code does not align with the location, claim type, or billing format. | Check CMS-1500 fields or UB-04 terms. |
| 11 | Diagnosis does not support the procedure | The payer sees a medical-necessity or diagnosis-linkage issue. | Review medical necessity criteria and documentation. |
| 16 | Missing or incomplete claim information | Data, documentation, identifiers, or required details were not complete enough to process. | Use a correction checklist tied to coding workflow terms. |
| 18 | Duplicate claim or duplicate service | The payer believes the service was already submitted or paid. | Compare claim history, frequency rules, and claims management terms. |
| 22 | Another payer may be primary | The claim needs coordination with Medicare, Medicaid, commercial, or secondary coverage. | Fix payer order using commercial billing terms and COB rules. |
| 29 | Timely filing deadline problem | The payer says the claim, correction, or appeal arrived too late. | Escalate quickly with proof of filing and claims reconciliation history. |
| 39 | Services denied because authorization or review requirements were not met | The payer required approval, review, or supporting evidence before payment. | Connect the denial to utilization review terms. |
| 45 | Charge exceeds payer fee schedule or allowed amount | The payer reduced the charge to contract, fee schedule, or maximum allowance. | Confirm expected reimbursement through accurate billing and reimbursement. |
| 50 | Service does not meet medical-necessity rules | Diagnosis, documentation, frequency, or coverage policy did not support payment. | Audit against medical necessity criteria. |
| 96 | Non-covered charge | The payer does not cover the billed service under the patient’s benefit or policy. | Check payer policy, ABN/notice rules, and EOB language. |
| 97 | Payment included in another service | The payer considers the service bundled, packaged, or already paid under another code. | Review coding edits and modifiers. |
| 109 | Claim not covered by this payer or contractor | The claim was routed to the wrong payer, plan, or contractor. | Fix eligibility and routing through electronic claims submission. |
| 119 | Benefit maximum reached | The patient’s plan limit, visit count, or benefit cap was reached. | Verify eligibility and benefits before rebilling. |
| 151 | Payer says documentation does not support the frequency or amount billed | The service may exceed payer frequency limits or medical record support. | Review documentation requirements. |
| 163 | Attachment or documentation was not received | Required records, forms, or attachments failed to reach the payer. | Rebuild proof using medical record retention terms. |
| 164 | Attachment or documentation arrived too late | The payer received supporting documents after the required window. | Track attachment deadlines inside the denial workqueue. |
| 165 | Referral issue | The referral was missing, expired, exceeded, or not aligned with plan requirements. | Connect referral controls to EHR integration terms. |
| 197 | Authorization or precertification missing | The payer required prior approval before the service was performed or billed. | Route to authorization follow-up and CDI review. |
| 204 | Service not covered under the current benefit plan | The plan does not cover the service for this member, setting, or benefit design. | Check eligibility, benefits, and payer policy before appeal. |
| 226 | Information from the billing provider was insufficient | The payer needs clearer data, records, coding support, or claim detail. | Use coding query process terms to close documentation gaps. |
| 234 | Service not separately payable | The payer bundled payment into another service, procedure, or allowance. | Review specialty edits, payer rules, and surgical coding compliance. |
| 236 | Procedure or procedure code was not paid separately | The payer’s reimbursement logic packaged the service with another payment. | Check edit logic before adding modifiers or appealing. |
| 243 | Service authorization or network process issue | The payer expected a specific referral, network approval, or managed-care process. | Connect payer rules with Medicaid billing software when applicable. |
| 252 | Additional documentation required | The payer needs more information before final processing or payment. | Build an attachment packet and monitor payer deadlines. |
| 253 | Sequestration or reduction-related adjustment | The payer applied a required payment reduction. | Post separately from payer denial categories and reconcile expected allowed amount. |
| 299 | Billing provider not eligible for payment | Provider enrollment, credentialing, taxonomy, or payer participation may be wrong. | Audit setup through credentialing organization terms. |
| 302 | Authorization time limit expired | The approval existed, but the allowed authorization window was missed. | Track approval date ranges inside the claim workflow. |
2. How to Read CARCs With Group Codes, RARCs, and EOB Language
A CARC should rarely be read alone. The group code tells the broad financial category, while the CARC explains the reason for the adjustment, and the RARC may add the missing detail that decides the next action. CMS states that some CARCs are too generic to communicate the reason clearly without at least one remark code, and RARCs further explain an adjustment or provide remittance processing information. A strong billing team reads the CARC beside remittance advice remark codes, EOB guidance, CARC definitions, and payment posting rules before assigning the balance.
The same CARC can create different actions depending on the group code. A deductible CARC with patient responsibility may move to patient billing or secondary filing. A medical necessity CARC with contractual obligation may require a provider write-off, appeal, or documentation review. A coordination CARC may need primary payer information before any appeal makes sense. A timely filing CARC may be appealable if the team has proof of original submission, clearinghouse acceptance, or payer portal confirmation. This is where clearinghouse terminology, EDI billing terms, electronic claims submission platforms, and claims reconciliation protect the team from appealing blindly.
The worst posting error is writing off a recoverable CARC as contractual because the payment “looked normal.” CARC 45, for example, may be a correct fee schedule adjustment, but it can also hide a payer underpayment if the wrong contract, locality, provider type, site of service, or modifier was applied. CARC 97 may be a correct bundled-service outcome, but it can also reveal missed modifier support or incorrect coding-edit logic. CARC 16 may be easy to correct if the missing field is obvious, yet disastrous if nobody identifies the missing element before the payer deadline. Every CARC should tie to medical coding workflow, coding edits and modifiers, medical coding audit terms, and billing reconciliation.
3. CARC Categories That Cause the Most Revenue Leakage
Eligibility and payer-routing CARCs usually begin at registration, not in billing. Wrong member ID, inactive coverage, incorrect plan selection, missing primary payer data, and managed care routing errors create avoidable work after the claim has already aged. CARC 22 and 109-type patterns should be reported back to front-end teams, not just corrected by back-end billers. If the same location keeps producing COB denials, the fix may live in eligibility workflow, payer mapping, or front-desk training. Teams should connect these patterns to COB guidance, commercial insurance billing, Medicaid billing software, and RCM software terms.
Coding and medical-necessity CARCs usually expose weak documentation-to-code alignment. CARC 11, 50, 97, 151, and 234 patterns should trigger code, modifier, diagnosis, order, note, and payer policy review. If coders only correct the claim without fixing the documentation habit, the denial will return next month with a different patient. This is especially painful in specialties with strict coding rules, including cardiology CPT coding, radiology billing, gastroenterology CPT codes, and orthopedic CPT coding.
Authorization and referral CARCs usually reveal broken handoffs. CARC 39, 165, 197, 243, and 302-type patterns show that approval, referral, precertification, notification, or date-range control failed somewhere before billing. These denials can be financially brutal because the service may have been clinically appropriate, documented, coded, and performed, yet still unpaid because a process requirement failed. Strong teams manage these through utilization review terms, clinical documentation improvement, medical necessity criteria, and problem list documentation.
Posting and contract CARCs are the quietest form of leakage because they often look like normal adjustment activity. CARC 45, sequestration-type adjustments, contractual reductions, bundled-payment reductions, and payer fee schedule variances require disciplined expected-versus-actual review. A payment poster should know when to accept the adjustment, when to send secondary, when to transfer patient responsibility, and when to escalate an underpayment. That workflow needs physician fee schedule terms, Medicare reimbursement, revenue cycle metrics, and data analytics reporting.
Quick Poll: Which CARC pattern is hurting your revenue cycle most?
4. CARC Root-Cause Workflow for Denials, Corrections, and Appeals
A CARC workflow should begin with classification. Put every adjustment into one of five buckets: patient responsibility, contractual adjustment, correction needed, appeal needed, or payer follow-up needed. This prevents staff from touching the same denial multiple times without progress. A CARC 1, 2, or 3 may be patient responsibility after COB is exhausted. A CARC 16 may require a corrected claim. A CARC 50 may require documentation appeal. A CARC 45 may require contract validation. A CARC 109 may require payer rerouting. The classification should connect to payment posting, claims reconciliation, denial management, and collections rules.
The second step is ownership. Registration should own eligibility, demographic, payer order, and COB defects. Coding should own code, modifier, diagnosis, bundling, and medical necessity defects. Clinical documentation teams should own note quality, missing signatures, incomplete orders, and payer evidence. Credentialing should own provider enrollment and billing eligibility. Payment posting should own contractual adjustment accuracy and underpayment variance. Compliance should own audit-risk patterns. This prevents the common failure pattern where every CARC lands in the same generic denial queue and nobody fixes the upstream behavior. Ownership should be reinforced through coding competency assessment, coding education terms, professional development terms, and coding ethics standards.
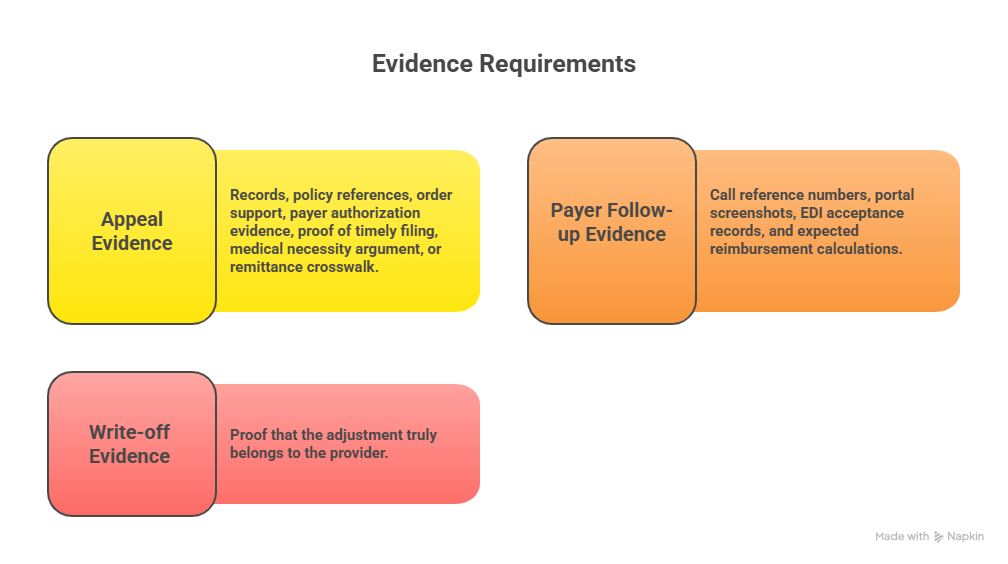
The third step is evidence. A corrected claim needs corrected data. An appeal needs records, policy references, order support, payer authorization evidence, proof of timely filing, medical necessity argument, or remittance crosswalk. A payer follow-up needs call reference numbers, portal screenshots, EDI acceptance records, and expected reimbursement calculations. A write-off needs proof that the adjustment truly belongs to the provider. Without evidence, CARC work becomes opinion work. Evidence control belongs inside medical record retention, EHR documentation terms, electronic data interchange, and medical billing reconciliation.
The fourth step is prevention. If the same CARC appears repeatedly, do not celebrate faster denial work. Fix the condition that creates the denial. Build claim scrubber edits for missing modifiers. Add front-end alerts for payer order. Create authorization date-range checks. Train providers on documentation phrases that support medical necessity. Update fee schedule tables. Tighten EVV-to-claim matching for home care. Prevention is the bridge between CARC analysis and lower denial rates, especially for teams using coding automation terms, encoder software terms, practice management system terms, and charge capture terms.
5. How to Build a CARC Dashboard That Actually Improves Cash
A useful CARC dashboard should show denial volume, denied dollars, recovered dollars, write-off dollars, appeal success rate, days to touch, days to resolution, payer frequency, location frequency, provider frequency, code frequency, and owner performance. A dashboard that only lists the top ten CARCs is too shallow. Leadership needs to know which CARCs are growing, which ones are preventable, which ones are recoverable, and which ones point to payer behavior rather than internal error. This turns CARC reporting into RCM KPI tracking, revenue cycle efficiency, coding productivity benchmarking, and revenue leakage analysis.
The dashboard should separate “high frequency” from “high financial impact.” CARC 1, 2, and 3 may appear often because patient responsibility is normal. CARC 50 may appear less often but carry high appeal value. CARC 29 may be lower volume but signals severe process failure because missed timely filing usually means lost recovery. CARC 45 may appear constantly, yet only some instances deserve underpayment review. CARC 197 may show that authorization workflow is failing before care is delivered. This analysis should connect to billing compliance violations, compliance audit trends, medical coding error rates, and impact of coding accuracy on revenue.
Training should come directly from CARC trends. If CARC 16 spikes, train staff on missing data patterns. If CARC 97 rises, train coders on bundling and modifier logic. If CARC 22 increases, train registration on payer order and benefit verification. If CARC 299 appears, audit provider enrollment setup. If CARC 50 appears by provider, run documentation education. This makes training precise instead of generic. It also supports exam prep and career development through medical coding certification terms, CBCS exam terms, continuing education units, and coding career development.
The dashboard should also respect official code updates. CMS tells MACs to update CARC and RARC lists based on the code update schedule, with publication updates occurring three times per year around March 1, July 1, and November 1, and CMS directs users to the official ASC X12 website for the complete code lists. That means billing software, denial rules, workqueue mappings, and training materials should be refreshed on a schedule. A stale CARC crosswalk can send staff down the wrong path, especially when deactivated, modified, or newly created codes affect payer remittance behavior.
6. FAQs About Claim Adjustment Reason Codes
-
Claim Adjustment Reason Codes are standardized codes used to explain why a claim or service line was paid differently from the billed amount. They appear on remittance advice and help billing teams understand whether the issue involves patient responsibility, payer contract rules, missing information, medical necessity, timely filing, coordination of benefits, or another adjustment reason. They should be read alongside RARC codes, EOB guidance, payment posting, and denial management.
-
CARCs are broader than denial codes because they explain payment adjustments, and an adjustment can mean denial, partial payment, reduced payment, patient responsibility, contractual adjustment, or additional payer action. CMS explains that remittance adjustments can include denied, zero payment, partial payment, reduced payment, penalty, additional payment, or supplemental payment situations. This is why billers should check the group code, CARC, RARC, payer policy, and claims reconciliation record before assigning the balance.
-
A CARC explains the core reason for the payment adjustment. A RARC gives additional explanation or remittance-processing detail when the CARC alone does not tell the full story. In practice, a CARC may say the claim lacks information, while the RARC may identify which documentation, field, or action is missing. Teams should connect both to CARC guidance, RARC guidance, EDI terms, and claims management.
-
Start with high-frequency and high-dollar patterns: deductible, coinsurance, copay, missing information, duplicate claim, COB, timely filing, contractual adjustment, medical necessity, non-covered charge, bundled service, missing authorization, missing documentation, and provider eligibility. Then group them by owner: registration, coding, documentation, authorization, credentialing, payment posting, or payer follow-up. This turns CARC review into revenue leakage prevention, RCM metrics, coding audit work, and billing compliance monitoring.
-
CARC 45 usually means the billed charge was reduced to a payer fee schedule, maximum allowance, or contracted amount. It should not be blindly written off until the payment team confirms the contract, fee schedule, place of service, modifier, provider status, and allowed amount. CARC 45 should be connected to physician fee schedule reimbursement, Medicare reimbursement, Medicaid reimbursement, and payment posting rules.
-
CARC 16 means the payer found the claim or service information incomplete. The team should read the RARC, identify the missing field or document, check whether the issue belongs to registration, coding, documentation, provider enrollment, or attachment workflow, and submit the corrected claim or missing evidence before the deadline. This workflow should use medical coding workflow terms, EHR documentation terms, coding query process terms, and medical record retention.