
Directory of Electronic Claims Submission Platforms
Electronic claims submission looks simple when a claim leaves the billing system. The real work sits underneath: payer enrollment, EDI routing, claim edits, documentation alignment, ERA posting, rejection handling, and reconciliation. A strong platform helps teams prevent silent revenue loss, while a weak setup turns clean work into delayed cash. This directory shows how to compare platform types, where each one fits, and which workflow gaps create the most expensive billing problems for practices using revenue cycle management software, clearinghouse workflows, EDI billing, and claims management.
1. How Electronic Claims Submission Platforms Fit the Revenue Cycle
Electronic claims submission platforms move billing data from the practice to the payer, yet the value comes from everything they catch before that handoff. A platform may validate patient demographics, check payer IDs, scrub diagnosis and procedure combinations, confirm NPI and taxonomy fields, route professional claims through CMS-1500 workflows, route institutional claims through UB-04 billing, and return payer responses that feed payment posting, claims reconciliation, and denial management.
The biggest buying mistake is treating submission as a send button. A weak platform may transmit claims successfully while leaving the team blind to front-end rejections, payer-specific edits, attachment failures, COB sequencing problems, or ERA mismatches. That is where practices leak revenue while believing the billing department is “caught up.” Teams need a platform that supports accurate medical billing and reimbursement, connects with practice management systems, protects EHR integration, and surfaces the right data for RCM metrics and KPIs.
A practical directory should separate platform categories by job. Clearinghouses handle routing, validation, payer connections, and 837 transaction flow. Practice management systems create, queue, edit, and track claims. EHR-integrated billing modules reduce duplicate entry when documentation, orders, coding, and charge capture connect cleanly. Payer portals help when a payer requires direct entry, claim status checks, authorization follow-up, or attachments. Denial platforms work after adjudication by organizing CARCs, RARCs, appeal steps, and payer behavior. Analytics platforms expose patterns across revenue leakage, medical billing reconciliation, coding errors, and coding denials management.
| Platform Type | Best Fit | Pain Point It Solves | Implementation Check |
|---|---|---|---|
| Core clearinghouse platform | Multi-payer routing and 837 transmission | Claims disappear between billing and payer intake | Confirm payer IDs, enrollment status, rejection reports, and clearinghouse terminology. |
| EDI gateway | Practices needing controlled transaction exchange | 837, 835, eligibility, and claim status files lack traceability | Map transaction workflows against EDI billing terms. |
| Practice management claim module | Small and mid-size practices | Charges, claims, payments, and balances sit in separate tools | Test integration with practice management systems. |
| EHR-integrated billing platform | Provider groups needing documentation-to-claim continuity | Codes, notes, orders, and charges fail to match | Audit the handoff using EHR integration terms. |
| RCM software suite | Organizations wanting end-to-end workflow control | Teams chase claims without shared work queues | Compare dashboards against RCM software terms. |
| Payer web portal | Direct claim entry, status checks, and attachments | A payer requires manual follow-up outside batch submission | Document portal steps inside coding workflow. |
| Medicare submission workflow | Practices with heavy Medicare volume | Coverage, documentation, and reimbursement checks happen too late | Pair submission review with Medicare reimbursement. |
| Medicaid claims platform | State Medicaid and managed Medicaid billing | State-specific rules keep creating preventable rework | Align setup with Medicaid billing software. |
| CMS-1500 professional claim tool | Physician, therapy, and outpatient professional billing | Field-level errors trigger payer intake rejections | Validate fields against CMS-1500 terms. |
| UB-04 institutional claim tool | Hospitals, facilities, hospice, and outpatient departments | Revenue codes, type of bill, and occurrence data create delays | Check mapping with UB-04 billing terms. |
| Claim scrubber/edit engine | Teams with high rejection or denial volume | Bad claims reach payers and return days later | Review edits against coding edits and modifiers. |
| Eligibility verification platform | Front desk, intake, and pre-claim checks | Coverage problems appear after care is delivered | Tie results to patient responsibility. |
| Prior authorization and attachment tool | Specialties needing documentation support | Claims stall because proof sits outside the submission workflow | Connect attachment rules with medical necessity criteria. |
| ERA/835 management module | Payment posting and remittance teams | Payments post incorrectly because remit data lacks structure | Standardize posting with payment posting terms. |
| CARC/RARC denial mapping tool | High-volume denial teams | Staff guess denial causes from vague payer messages | Use CARCs and RARCs. |
| Secondary billing and COB platform | Practices with Medicare secondary or complex payer sequencing | Claims deny because payer order is wrong | Build rules from COB definitions. |
| Claims reconciliation dashboard | Billing managers tracking claim lifecycle gaps | Submitted, accepted, denied, paid, and adjusted claims lack one source of truth | Measure outcomes through claims reconciliation. |
| Denial management platform | Teams with recurring preventable denials | Appeals happen one claim at a time with no root-cause learning | Compare against denial management services. |
| Revenue leakage analytics | Leadership reviewing cash gaps and underpayment | Lost revenue hides inside adjustments, write-offs, and stale AR | Track leakage using revenue leakage analysis. |
| Specialty billing platform | Cardiology, radiology, GI, dermatology, ambulance, and lab billing | Generic edits miss specialty-specific billing risk | Match claim rules to cardiology CPT, radiology CPT, and ambulance coding. |
| Telemedicine claims workflow | Virtual care and hybrid practices | Place of service, modifier, payer policy, and documentation mistakes multiply | Use telemedicine coding terms. |
| Commercial insurance submission tool | Practices with many plan rules and contracts | Each payer behaves differently and staff memorize workarounds | Standardize payer notes with commercial insurance billing. |
| Patient balance and estimate platform | Groups wanting cleaner post-adjudication collection | Patients receive confusing balances after payer processing | Align estimates with copay and patient responsibility. |
| Small-practice billing platform | Independent practices needing simple queues and reporting | Staff wear too many hats and miss aging claim signals | Compare options in small-practice billing solutions. |
| Automation-assisted claims platform | Teams wanting fewer repetitive manual tasks | Manual claim checks consume staff time while errors still pass through | Define guardrails with coding automation terms. |
| Compliance-focused claims platform | Organizations under audit pressure | Claim submission lacks an audit trail for edits, changes, and approvals | Pair workflow controls with coding regulatory compliance. |
| Data analytics and reporting layer | Managers comparing payer behavior and staff performance | Submission data exists, yet nobody can turn it into decisions | Build reports from data analytics terms. |
| Security-centered billing platform | Remote or distributed billing teams | Access controls, file transfers, and PHI handling become weak points | Review safeguards with healthcare data security. |
| Managed billing and submission service | Practices outsourcing some or all billing operations | Internal capacity, training, and follow-up discipline cannot keep up | Compare service scope against RCM terms and claims management terms. |
2. How to Choose the Right Platform Type
The right platform depends on where your claim process breaks. If the team struggles with payer routing, enrollment, claim acceptance, and front-end rejections, start with the clearinghouse layer and review clearinghouse terminology, EDI billing terms, and electronic claims submission platforms. If the team struggles before submission because charges, notes, codes, and provider sign-off do not align, the platform decision belongs closer to EHR documentation, EMR documentation terms, clinical documentation improvement, and charge capture.
A small practice with low claim volume may need a clean practice management system, eligibility checks, a reliable clearinghouse connection, and tight payment posting. A specialty group may need a platform that understands modifiers, payer edits, procedure-to-diagnosis logic, attachments, and payer policy differences. A hospital outpatient department needs stronger facility billing controls, revenue code logic, UB-04 discipline, and reconciliation. The practical question is simple: where does money get trapped? If money gets trapped before submission, review medical coding workflow, medical necessity criteria, problem lists in documentation, and SOAP notes and coding. If money gets trapped after adjudication, prioritize CARC analysis, RARC analysis, claims reconciliation, and payment posting.
The best selection process begins with a 30-day claim failure review. Pull rejections, denials, late payments, underpayments, no-response claims, attachment requests, eligibility-related write-offs, secondary billing problems, and manual portal work. Group each issue by root cause: intake, eligibility, coding, documentation, charge capture, payer enrollment, EDI routing, payer edit, adjudication, remittance, or follow-up. That turns a vague software search into a buying checklist tied to RCM KPIs, revenue leakage prevention, coding accuracy and hospital revenue, and medical coding error rates.
3. Platform Features That Actually Protect Reimbursement
A platform earns its place when it prevents predictable failure. Strong electronic claims submission should provide payer-specific edits, eligibility integration, batch status tracking, rejection queues, audit trails, attachment workflows, ERA import, secondary billing support, denial code grouping, and reconciliation reporting. These features protect reimbursement because they force the team to resolve issues while the claim is still actionable. That is why submission needs to connect with accurate reimbursement, claim adjustment reason codes, remittance advice remark codes, and medical billing reconciliation.
Payer enrollment support deserves special attention. A beautiful dashboard means very little when claims fail because an NPI, TIN, taxonomy, group number, provider enrollment file, or payer submitter ID is wrong. The platform should show which payers are live, which require enrollment, which support ERA/EFT, and which require portal steps. Billing teams should also keep a payer setup log that ties each payer to claim format, submitter ID, authorization rules, secondary billing behavior, timely filing limits, and attachment requirements. That documentation helps protect commercial insurance billing, Medicare reimbursement, Medicaid billing software, and provider fee schedule reimbursement.
The second feature group is edit intelligence. Generic claim scrubs catch missing fields, yet payer behavior usually demands more nuance. A strong platform should flag diagnosis mismatch, modifier conflicts, place-of-service conflicts, invalid provider taxonomy, duplicate claims, global period risk, bundling issues, and documentation-sensitive codes. Specialty billing teams need edits connected to CPT modifiers, surgical coding compliance, radiology billing, lab and pathology coding, and telemedicine coding.
The third feature group is reporting that drives action. A dashboard should show acceptance rate, rejection rate, denial rate, days to first payer response, claims without response, payer turnaround, denial category, underpayment risk, adjustment patterns, and staff queue aging. If the report only counts submitted claims, leadership gets activity metrics instead of revenue protection. A stronger setup connects submission data with data analytics and reporting, RCM efficiency benchmarks, coding productivity benchmarks, and compliance audit trends.
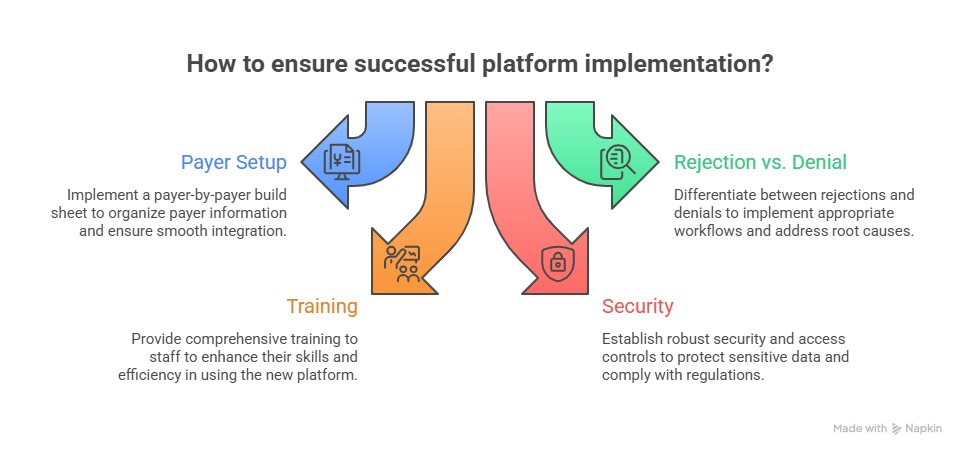
4. Implementation Mistakes That Create Expensive Submission Problems
Platform implementation fails when the team transfers old habits into a new system. If payer setup is messy, the new platform only moves messy work faster. If claim edits are ignored, preventable errors still reach the payer. If ERA posting is poorly mapped, payment data creates downstream cleanup. The implementation plan should begin with a payer-by-payer build sheet that includes payer ID, claim format, submitter enrollment, ERA enrollment, EFT status, attachment method, authorization method, secondary billing rules, and denial contacts. That build sheet should connect to healthcare claims management, RCM terms, billing acronyms, and medical abbreviations.
Another costly mistake is treating rejections and denials as the same problem. A rejection usually means the claim failed before payer adjudication or intake acceptance. A denial usually means the payer accepted the claim and then refused payment after applying policy, coverage, coding, documentation, or benefit rules. Teams that mix the two lose root-cause clarity. Rejection workflows belong with clearinghouse edits, payer IDs, demographic accuracy, NPI/TIN setup, and required fields. Denial workflows belong with CARCs, RARCs, medical necessity, and utilization review.
Training also gets underestimated. Staff should know how to read rejection reports, correct claim-level errors, escalate enrollment issues, identify payer-system outages, separate provider setup errors from coding errors, and document follow-up actions. A coder may see a modifier issue; a biller may see a payer edit; a payment poster may see an adjustment trend; a manager may see a revenue leak. A strong platform helps each role act quickly. A strong training plan reinforces coding competency, medical coding audit terms, compliance standards, and medical coding regulatory compliance.
Security and access controls deserve early planning. Claims submission touches PHI, payment data, provider credentials, user permissions, audit trails, and sometimes remote work. The platform should support role-based access, secure file exchange, user activity logs, and clean offboarding. Billing leaders should review user permissions by role: front desk, coder, charge entry, biller, payment poster, supervisor, provider, and outside vendor. This protects healthcare data security, HIPAA-related billing risk, record retention, and remote billing workforce controls.
5. A Practical Shortlist Method for Comparing Platforms
A useful shortlist should score platforms against real workflow pressure. Start with seven categories: claim creation, pre-submission editing, payer enrollment, batch transmission, rejection handling, remittance posting, and reporting. Give each category a score from 1 to 5 using live examples from your own claims. A platform demo becomes much more honest when the vendor must show how the tool handles a denied telemedicine claim, a COB issue, a Medicare secondary claim, a missing authorization, a payer ID problem, and an ERA underpayment. Those examples connect the buying decision to COB terms, telemedicine billing, Medicare documentation, and underpayment reconciliation.
Ask each platform vendor to demonstrate three workflows without slides: submit a corrected professional claim, resolve a front-end rejection, and post an ERA with adjustment codes. Watch how many screens, exports, manual notes, and outside portals are needed. A clean platform should show claim history, payer response, user action, correction reason, resubmission date, and next follow-up. It should also help managers find stale claims, repeated rejections, recurring denial categories, and staff queue bottlenecks. Those capabilities support billing compliance violations prevention, impact of accurate coding on reimbursement, coding denials best practices, and RCM efficiency analysis.
Pricing should be reviewed through total operating cost, not subscription cost alone. Look at per-claim fees, payer enrollment fees, ERA fees, support fees, implementation fees, data migration costs, training time, clearinghouse pass-through costs, portal work that remains manual, and reporting gaps that require spreadsheets. A cheaper system can become expensive when staff spend hours fixing preventable rejections or reconciling mismatched payments. Use claim volume, denial volume, labor hours, days in AR, and write-off patterns to compare options. That connects platform value to collections and bad debt, patient responsibility, revenue leakage prevention, and hospital reimbursement rates by specialty.
The final shortlist should include one operational owner for each risk area. Billing owns claim queues. Coding owns code accuracy and edit response. Front desk owns eligibility and demographics. Payment posting owns ERA mapping. Compliance owns audit trail and access controls. Leadership owns reporting and revenue impact. When ownership is clear, the platform becomes a control system rather than another tool staff blame when claims age. That ownership model also strengthens professional development, career development, coding education and training, and CBCS exam readiness.
6. FAQs About Electronic Claims Submission Platforms
-
A clearinghouse is one major type of electronic claims submission platform. It routes claims, validates transaction data, manages payer connections, and returns acceptance or rejection messages. A broader submission platform may include clearinghouse access plus practice management, claim scrubbing, eligibility, payer enrollment, ERA posting, denial queues, and analytics. Teams should compare both the routing layer and the workflow layer using clearinghouse terms, EDI billing terms, RCM software terms, and claims management terms.
-
A small practice usually needs a practice management system with integrated clearinghouse submission, eligibility verification, rejection tracking, ERA posting, and simple AR reporting. The best choice depends on payer mix, claim volume, specialty, staff capacity, and denial patterns. A lean setup should still protect CMS-1500 claims, payment posting, small-practice billing solutions, and accurate reimbursement.
-
It should show batch status, payer acceptance, clearinghouse rejection, payer rejection, claim status, follow-up owner, ERA response, adjustment code, payment posting status, and reconciliation outcome. A submitted claim with no response should trigger workqueue attention before timely filing risk grows. Strong teams connect this reporting with claims reconciliation, CARC tracking, RARC tracking, and RCM KPIs.
-
They reduce denials by catching preventable issues before the payer adjudicates the claim. Valuable controls include eligibility checks, payer-specific edits, diagnosis-to-procedure validation, modifier review, documentation prompts, authorization reminders, duplicate claim alerts, and attachment tracking. Denial reduction also depends on human review, coding judgment, and clear escalation paths. The platform should support medical necessity checks, coding edits and modifiers, denial management, and coding compliance.
-
Clean provider demographics, NPI, TIN, taxonomy, payer IDs, fee schedules, location records, place-of-service rules, modifier rules, eligibility workflows, claim templates, ERA enrollment, EFT enrollment, user permissions, and payer contact lists. Also review open AR, recurring denials, and payer-specific workarounds before migrating workflows. This protects practice management systems, EHR integration, charge capture, and healthcare data security.
-
Measure success through rejection rate, denial rate, first-pass acceptance rate, days to payer response, days in AR, clean claim rate, payment posting lag, unresolved claim volume, underpayment findings, staff queue aging, and revenue leakage. The best metric set shows whether the platform improved cash, reduced rework, and strengthened accountability. Managers should connect these outcomes with revenue cycle metrics, revenue leakage insights, RCM efficiency benchmarks, and data analytics reporting.