
Hierarchical Condition Categories (HCCs): Coding Definitions
Hierarchical Condition Categories, usually shortened to HCCs, sit at the center of risk-adjusted reimbursement because they turn documented chronic disease burden into a structured payment signal. If coders, billers, auditors, and CDI teams misunderstand the terminology, organizations do not just lose reimbursement accuracy. They lose forecasting accuracy, compliance control, RAF integrity, and the ability to defend why a patient population is more complex than it looks on a fee-for-service claim.
This guide breaks HCC terminology into practical language that billing and coding teams can actually use. You will see what each term means, why it matters operationally, where the most expensive mistakes happen, and how HCC work connects with risk adjustment coding, clinical documentation integrity, medical necessity criteria, medical coding audits, and regulatory compliance.
1. What HCC Coding Actually Means in Medical Billing
HCC coding is the process of capturing clinically supported diagnoses that roll up into risk-adjustment categories used to estimate future healthcare cost burden. That sounds abstract until you see what it changes in real operations. HCCs affect how payers view population complexity, how providers are compared against peers, how suspected chronic conditions are followed up, and how accurately organizations can align reimbursement with disease burden. This is why HCC work belongs beside risk adjustment coding, clinical documentation improvement terms, SOAP notes and coding, EHR coding terms, and problem lists in medical documentation.
The key operational truth is that HCCs are not built from vague patient history. They are built from specific diagnosis reporting backed by current-year documentation, assessment, and management. That means teams cannot treat HCC capture like a passive export from the chart. They need disciplined diagnosis review, provider education, and strong query practices supported by the coding query process, accurate clinical documentation guidelines, medical record retention and storage terms, medical coding workflow terms, and coding audits.
This is where many teams fail. They report diagnoses that were copied forward but never truly addressed. Or they miss diagnoses that were clinically obvious but not documented to the standard needed for coding. Or they let generalized diagnosis language flatten severity, which collapses the patient’s true risk profile. Those misses affect more than one claim. They damage the entire risk picture. Strong HCC performance depends on the same discipline behind CDI programs, medical coding automation oversight, revenue leakage prevention, coding compliance trends, and impact of coding accuracy on revenue.
HCC coding also requires a different mindset from traditional procedure-driven billing. In a fee-for-service mindset, the focus is often whether the service line will pay. In an HCC mindset, the focus is whether the full clinical burden was captured with defensible precision. That requires teams to connect diagnosis specificity with medical necessity, documentation standards, coding education and training, HIPAA-compliant documentation handling, and medical coding career development. HCCs reward disciplined clinical truth, not diagnosis inflation and not passive chart clutter.
| Term | What It Means | Why It Matters | Best Practice Action |
|---|---|---|---|
| HCC | A grouped risk category built from qualifying diagnoses | Turns documented disease burden into payment-relevant risk data | Validate that diagnosis specificity supports category assignment |
| Risk Adjustment | Method of adjusting payment based on patient illness burden | Prevents complex patients from looking artificially cheap | Tie diagnosis capture to population cost forecasting |
| RAF Score | Risk adjustment factor derived from demographics and diagnoses | Influences the reimbursement signal attached to patient complexity | Review major RAF shifts for documentation or coding causes |
| ICD-10-CM Code | Diagnosis code set used to report conditions | The code is the bridge between documentation and HCC logic | Code to highest supported specificity |
| Mapped Diagnosis | A diagnosis that links to a recognized HCC category | Not every diagnosis affects risk adjustment | Use mapping review before year-end sweeps |
| Non-Mapped Diagnosis | A diagnosis that does not create an HCC | Still clinically important but does not change risk score directly | Do not confuse clinical relevance with HCC value |
| Hierarchy | Rule where a more severe condition overrides a related lower one | Prevents stacking related severity levels incorrectly | Audit grouped conditions for severity logic |
| Severity Capture | Documentation that reflects true disease seriousness | Flat documentation can collapse higher-risk categories | Educate providers on specificity language |
| MEAT | Monitor, Evaluate, Assess, Treat evidence for a diagnosis | Supports whether a condition is actively managed and reportable | Look for at least one defensible care activity in the note |
| Problem List | Chart list of ongoing or historical diagnoses | Helpful starting point but not enough by itself for coding | Confirm active note support before coding from it |
| Chronic Condition | Ongoing disease requiring continued management | Core driver of many HCC categories | Track annual recapture with provider workflows |
| Recapture | Re-reporting a qualifying condition in the current year | Past-year coding does not automatically carry forward | Use annual outreach and chart prep processes |
| Suspect Condition | A likely chronic diagnosis not yet confirmed in current documentation | Helps focus chart review and provider follow-up | Never code from suspicion alone |
| Gap Closure | Resolving an open condition capture opportunity | Improves diagnosis completeness and risk accuracy | Match chart prep lists to visit workflows |
| Face-to-Face Encounter | Provider-patient visit supporting diagnosis reporting | Supports defensible current-year diagnosis capture | Verify encounter type eligibility for risk reporting rules |
| Assessment | Provider statement recognizing the condition | A diagnosis must be clearly documented, not implied | Query when clinical language is ambiguous |
| Specificity | Level of diagnostic detail documented and coded | Better specificity protects both compliance and risk accuracy | Avoid unspecified codes when support exists |
| Combination Code | Single code capturing multiple related clinical facts | May better represent severity and mapping | Review when diabetes, CKD, or vascular links exist |
| Unsupported Diagnosis | Condition coded without sufficient note support | Creates audit exposure and credibility loss | Hold until documentation is corrected or clarified |
| Upcoding Risk | Reporting greater severity than the note supports | Compliance failure with repayment and audit consequences | Use second-level review for high-impact diagnoses |
| Undercoding Risk | Failing to capture supported complexity | Suppresses true patient burden and revenue accuracy | Audit recapture misses and provider education patterns |
| Validation Review | Check that diagnosis, note, and code all agree | The core compliance step in HCC coding | Require coder-auditor feedback loops |
| Retrospective Review | Chart review after the encounter occurred | Finds missed HCC opportunities but can be slower | Use for trend analysis and audit cleanup |
| Prospective Review | Chart prep before the encounter | Raises the odds that chronic conditions are addressed in real time | Build pre-visit suspect lists carefully |
| Recoding | Correcting a diagnosis assignment after review | Prevents unsupported or incomplete HCC reporting from persisting | Document correction rationale clearly |
| Deletion | Removing a diagnosis that should not have been reported | Essential when a note does not support active reporting | Track deletion reasons for training use |
| Annual Reset | Need to capture qualifying conditions again each year | Past coding does not guarantee current risk recognition | Monitor open recapture gaps monthly |
| Audit Trail | Documentation showing how and why the diagnosis was coded | Protects the organization during payer or regulatory review | Retain note, code logic, and reviewer comments |
| Diagnosis Refresh | Updating stale condition language to current clinical truth | Old vague labels weaken coding precision | Coach providers to document active status and severity |
| Coding Governance | Oversight structure for quality, audit, and education | Keeps HCC performance from drifting into unsafe shortcuts | Set ownership for audit, education, and remediation |
2. The Core HCC Definitions Every Coder, Auditor, and CDI Team Must Know
The first definition that matters is hierarchy itself. HCC systems do not simply add every related condition together. They use severity logic so the more serious form of a related disease family overrides the less serious form. That prevents artificial stacking, but it also means vague coding can depress the patient’s captured burden. Teams working in this space must understand severity the same way they understand coding edits and modifiers, ICD-11 best practices, medical coding audit terms, regulatory compliance, and medical coding error patterns.
The next essential definition is recapture. HCC coding is not a permanent badge attached to the chart. Qualifying chronic conditions need to be supported and reported again in the current year. That single fact explains why so many organizations see sharp swings in risk scores even when their patient population did not suddenly become healthier. If teams do not run deliberate recapture workflows using EMR documentation terms, EHR integration terms, problem list management, encoder software terms, and medical billing software solutions, supported conditions go silent.
Another foundational definition is MEAT-style support, meaning some defensible evidence that the provider monitored, evaluated, assessed, or treated the condition. The exact documentation culture may vary, but the core principle does not. A diagnosis must be more than a copied artifact. It must be part of the visit’s actual clinical work. This is where HCC coding intersects tightly with clinical documentation integrity, essential documentation guidelines, medical necessity criteria, coding query process terms, and medical coding audits. The diagnosis must be visible, active, and clinically defensible.
Specificity is another definition that separates average HCC programs from strong ones. A chronic condition that is documented vaguely often loses severity, relationships, or manifestations that drive more accurate mapping. This matters for diabetes, vascular disease, renal disease, heart failure, and other multi-layered conditions. Coders need the same sharp specificity habits they would use in cardiology CPT coding, lab and pathology coding, radiology coding terms, surgical coding compliance, and telemedicine coding guidance. Precision protects both reimbursement integrity and compliance credibility.
Finally, teams need to understand the difference between a suspect condition and a reportable diagnosis. A suspect list is a workflow tool, not a coding permission slip. It tells the organization where to look, not what to submit. That boundary matters because HCC pressure can tempt teams into coding from inference rather than documentation. The guardrails come from ethical billing principles, HIPAA compliance in billing, compliance audit trends, billing compliance violations, and medical coding education accreditation. Good HCC work is aggressive about accuracy, not aggressive about unsupported capture.
3. How HCC Capture Breaks Down in Real Documentation and Coding Workflows
The most common HCC breakdown is the stale chart problem. Chronic conditions appear on the problem list year after year, so everyone assumes they are safely represented. But a problem list is not the same as an actively supported diagnosis in the current encounter. When providers rely on carried-forward templates, and coders rely on carried-forward impressions, the organization creates a false sense of security. Strong HCC workflows need chart review discipline supported by problem list guidance, SOAP note standards, EMR documentation terms, medical record retention terms, and accurate documentation practices. If the note does not prove current management, the diagnosis cannot safely carry the HCC burden.
The second failure point is flattened specificity. Providers may document “diabetes,” “heart disease,” “depression,” or “renal impairment” when the actual chart supports a much more precise clinical picture. That weak language can erase complication status, severity, manifestations, or relationships that matter for HCC mapping. Coders who do not query or educate around those patterns leave supported value behind. The fix requires the same analytic thinking used in ICD-11 coding for mental health, neurological disorder coding, respiratory disease coding, infectious disease coding, and oncology coding case studies. The disease family matters, but the documented clinical detail matters even more.
The third breakdown is overreliance on technology without governance. Encoder tools, suspecting tools, and EHR prompts can support HCC workflows, but they can also create lazy coding habits if teams assume every prompt is right. Technology should raise questions, not answer them automatically. That is why HCC programs need oversight built from encoder software terms, coding automation terms, RCM software terminology, billing practice management system terms, and future billing software trends. Automation without validation is just faster risk.
The fourth breakdown is the “visit happened, so code it” mindset. HCC work is not a reward for scheduling high-risk patients. It depends on whether the conditions were actually assessed or managed during the encounter. Teams under production pressure sometimes collapse that distinction. They assume the condition remains active, therefore reportable. That is where compliance risk enters. The safe standard is shaped by medical coding regulatory compliance, coding compliance trends, medical coding audits, billing compliance penalties, and ethical medical billing. A note must prove that the condition belonged in the coded picture for that year.
The fifth breakdown is poor ownership. HCC performance usually falls apart when everyone assumes someone else is watching it. Providers think coders will infer what matters. Coders think CDI will fix the note. Auditors think analytics will catch the misses. Analytics assumes operations has closed the gaps. The result is a quiet loss of RAF accuracy, weak recapture rates, and avoidable audit vulnerability. Strong ownership needs the same structure used in revenue cycle management, revenue cycle KPIs, coding productivity benchmarks, workforce shortage analysis, and future skills for medical coders. HCC success is a managed system, not a side project.
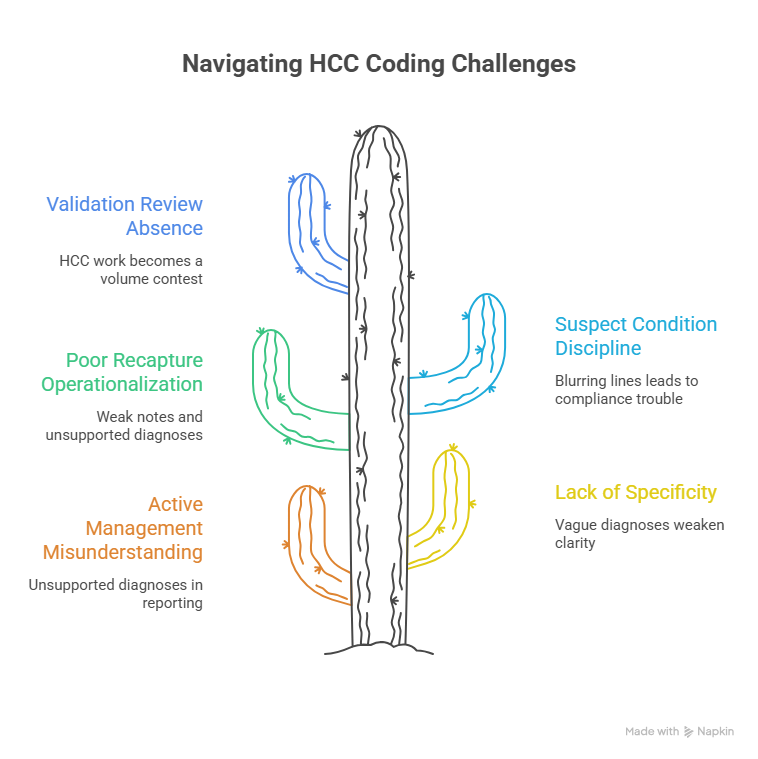
4. The HCC Terms That Separate Accurate Risk Capture From Compliance Trouble
The most dangerous term to misunderstand is active management. Many charts mention chronic disease history, but not every mention supports coding. If the provider did not monitor, evaluate, assess, or treat the condition in a way the record can defend, the diagnosis may not belong in the current reporting picture. That is why active management needs to be interpreted with the same discipline applied to clinical documentation integrity, medical necessity, CDI terms, coding query rules, and documentation guidelines. Coding a condition because it is true is not enough. It must also be currently supported.
Another make-or-break term is specificity. In HCC work, unspecified language does more than weaken clinical clarity. It can distort the patient’s modeled burden. A vague diagnosis may still tell part of the truth, but not the operationally useful part. If a condition has a documented manifestation, relationship, stage, severity, or complication, that detail matters. Teams that understand specificity at this level usually also perform better in radiology coding, emergency medicine CPT coding, orthopedic surgery CPT coding, dermatology CPT coding, and pediatric coding reference work. Precision is a habit, not a specialty-specific trick.
Recapture is another term that causes expensive confusion. Many organizations know the word, but operationalize it poorly. They wait until late in the year, scramble through stale suspect lists, and then pressure providers to validate everything in sight. That is how weak notes and unsupported diagnoses get created. Real recapture work is steady, targeted, and built into visit preparation, coder review, CDI follow-up, and audit feedback. It works best when connected to coding workflow terms, billing and reimbursement accuracy, revenue leakage prevention, revenue cycle efficiency benchmarks, and predictive analytics in medical billing. Recapture should feel like system design, not year-end panic.
Suspect condition is another term that demands discipline. A suspect diagnosis exists to trigger review, not to authorize coding. When organizations blur that line, compliance trouble follows. Coders must know when a suspect should become a provider query, when it should remain an analytic flag, and when it should be discarded entirely. That discipline is strengthened by coding audit practices, regulatory compliance guidance, ethical billing standards, HIPAA compliance changes, and medical coding education terms. High-performing teams are aggressive about review opportunities and conservative about unsupported coding.
Finally, validation review is the term that keeps HCC programs honest. Validation means the diagnosis, note, code choice, severity logic, and category impact all align. It is the step that protects organizations from both overstatement and understatement. Without validation review, HCC work turns into a volume contest. With it, HCC work becomes a disciplined representation of disease burden. That review is strongest when paired with medical coding audit terminology, billing compliance trend monitoring, impact of accurate coding on reimbursement, coding productivity benchmarks, and future-proof coding skills. Validation is where accuracy stops being a slogan and becomes a control.
5. Best Practices for Building an HCC Coding Process That Holds Up Under Audit
Start with provider-facing documentation design, not just coder education. HCC accuracy rises when providers know exactly what makes a chronic condition reportable in the current year. That means teaching them to document status, severity, related manifestations, and active management in language coders can defend. The best programs connect provider education with CDI guidance, documentation standards, query process rules, EHR documentation terms, and clinical documentation dictionaries. Coder excellence cannot fully compensate for vague provider language.
Next, build prospective review into the workflow. The best time to close HCC gaps is before or during the encounter, not months later in retrospective cleanup. Pre-visit chart prep, suspect list review, and focused condition prompts can make visits more accurate without turning them into documentation marathons. That infrastructure becomes easier when paired with EHR integration terms, practice management system terms, automation terms, revenue cycle software terms, and medical billing workflow guidance. A good system makes accurate capture easier at the point of care.
Then create a two-level review model for high-impact diagnoses. Conditions with meaningful category impact, high audit sensitivity, or repeated provider ambiguity should receive heightened validation. That is where audit resources generate real value. Use a structure informed by medical coding audits, compliance audit trends, coding error analysis, billing compliance penalties, and medical coding audit terms. Not every chart needs the same intensity, but the most consequential diagnoses do.
Measure the right HCC performance indicators. Many teams track only final RAF change, which is too late and too blunt. Better indicators include prospective review completion, suspect-to-supported conversion rate, recapture completion rate, unspecified diagnosis rate in mapped conditions, query response yield, unsupported diagnosis deletion rate, and audit agreement rate. Those indicators make more sense when read beside revenue cycle KPIs, RCM efficiency benchmarks, coding workforce analysis, remote workforce trends, and future coding roles. What gets measured gets taught, and what gets taught gets coded more consistently.
Finally, use HCC findings to strengthen the whole documentation and coding environment. The smartest organizations do not treat HCC misses as isolated misses. They use them to improve provider templates, coder education, pre-bill edits, audit targeting, and analytics logic. That feeds long-term resilience across medical coding career development, continuing education for coders, credentialing organizations, certification exam prep resources, and how continuing education accelerates coding careers. HCC excellence is not a separate island. It is a stress test for the quality of the entire coding operation.
6. FAQs About Hierarchical Condition Categories (HCCs)
-
An HCC is a diagnosis-based risk category that helps translate documented disease burden into a structured payment signal. It does not replace coding fundamentals. It depends on them. That is why HCC understanding fits naturally beside risk adjustment coding, clinical documentation integrity, medical necessity criteria, coding workflow terms, and medical coding regulatory compliance.
-
No. Many diagnoses are clinically relevant but do not map to an HCC category. That is why coders need to distinguish between overall diagnosis accuracy and diagnosis lines that directly affect risk adjustment. This becomes clearer when teams understand medical coding audit terms, ICD-11 best practices, problem list management, EHR coding terms, and encoder software use.
-
Because qualifying chronic conditions usually need current-year support and reporting. Last year’s accurate diagnosis does not automatically protect this year’s risk picture. Recapture matters most when tied to prospective workflow design, documentation standards, query process rules, CDI practices, and revenue leakage prevention.
-
A problem list is useful, but by itself it is not enough. The current note still needs to support that the diagnosis was actively addressed in a way the organization can defend. That standard becomes easier to apply when teams use SOAP note guidance, EMR documentation terms, medical record retention standards, clinical documentation dictionaries, and medical coding audits.
-
The biggest risk is reporting a diagnosis with more severity or certainty than the documentation supports. That includes coding from assumptions, copied-forward language, or suspect lists that were never validated. The strongest guardrails come from ethical billing principles, billing compliance penalty analysis, compliance trend monitoring, HIPAA compliance guidance, and coding audits.
-
A strong HCC program combines provider education, prospective chart prep, coder validation, focused auditing, and performance measurement. It also treats HCC gaps as documentation and workflow problems, not just coder misses. That kind of system improves fastest when connected to revenue cycle management, revenue cycle KPIs, coding productivity benchmarks, future skills for coders, and continuing education strategies.