
Guide to Medical Coding Apprenticeship & Internship Terms
Breaking into coding through an apprenticeship or internship sounds straightforward until you realize the real challenge is not just learning code sets. It is learning the language that governs supervision, productivity, documentation quality, claim accuracy, compliance risk, reimbursement impact, and hiring readiness. New coders often lose confidence because they can memorize definitions yet still struggle to interpret how training terms affect live work, audit exposure, and revenue outcomes.
This guide turns apprenticeship and internship terminology into practical operating knowledge. You will see what each term means, why employers care, where beginners get trapped, and how to use these concepts to become a safer, faster, more hireable coder.
1. Why apprenticeship and internship terms matter more than beginners expect
Many beginners enter training believing success depends on memorizing the material in a medical coding certification terms dictionary, studying a dictionary of terms for coding education and training, reviewing coding competency and assessment terms, and understanding guide to coding career development essential terms. Those resources matter, but apprenticeship performance is shaped by something more operational: whether you understand how training language connects to claim risk, audit exposure, workflow friction, and employer trust.
For example, a trainee may hear “productivity benchmark” and think it simply means speed. In real departments, productivity without judgment creates rework, avoidable denials, and hidden supervision costs. That is why training leaders evaluate you through the lens of medical coding workflow terms complete reference, revenue cycle management RCM terms explained, guide to healthcare claims management terms, and revenue cycle metrics and KPIs terms and definitions. They want proof that your work holds up after it leaves your desk.
That distinction separates trainees who look polished in class from trainees who become employable in production. Employers trust interns who can connect documentation to medical necessity criteria essential coding guide, link coding decisions to guide to accurate medical billing and reimbursement, recognize where medical coding audit terms comprehensive dictionary principles apply, and understand how errors become guide to claim adjustment reason codes CARCs or remittance advice remark codes RARCs comprehensive dictionary problems.
The smartest way to approach an apprenticeship is to treat terminology as workflow intelligence. Each term tells you what supervisors measure, what payers punish, what auditors question, and what hiring managers reward. When you interpret training terms through guide to medical coding regulatory compliance, complete guide to coding ethics and standards, guide to health information management HIM terms, and healthcare data security terms for medical coders, you start thinking like someone safe to hire.
| Term | What It Means | Why It Matters in Training | Best Practice Action |
|---|---|---|---|
| Apprenticeship | Structured earn-and-learn pathway with supervised skill building | Shows employers you trained in real workflows, not theory only | Ask how cases, feedback, and evaluations are sequenced |
| Internship | Shorter experience focused on exposure, practice, and readiness | Quality varies widely by site and supervisor | Confirm chart access, case mix, and review frequency |
| Preceptor | Experienced coder who reviews and coaches trainee work | Your learning speed depends heavily on preceptor quality | Track recurring corrections and build a personal error log |
| Shadowing | Observing coder workflow before coding independently | Helps trainees see decision logic, not just final answers | Take notes on query triggers, edits, and documentation gaps |
| Case Review | Line-by-line evaluation of coded records | Finds logic gaps before they become productivity habits | Request explanation for every downgrade or deleted code |
| Dual Coding | Trainee and trainer code the same chart for comparison | Fastest way to expose reasoning differences | Compare not only code choice but sequencing rationale |
| Audit Trail | Record of actions, changes, and review decisions | Protects both trainee and employer during quality disputes | Document what was changed and why |
| Turnaround Time | Expected time to complete assigned charts | Training fails when speed is pushed before judgment matures | Improve pace only after accuracy stabilizes |
| Accuracy Rate | Percentage of charts coded correctly | Core hiring and advancement metric | Measure by error type, not one blended score alone |
| Productivity Benchmark | Target output for chart volume or complexity | Shows when trainee can handle real workload | Ask whether benchmark is adjusted for specialty and case type |
| Escalation | Routing unclear cases to a senior coder or lead | Safe escalation prevents guess-based coding | Escalate ambiguity before claim submission |
| Query | Formal request for provider clarification | Critical when documentation does not support code choice | Know when to query versus when documentation is simply insufficient |
| Denial | Claim rejected or reduced by payer | Training quality is visible in denial patterns | Study denial root causes, not denial labels only |
| Medical Necessity | Service must be clinically justified per payer rules | A correct code can still fail payment | Link documentation support to billed services |
| Modifier | Code addition that clarifies service circumstances | Heavy error area for trainees | Learn payer-sensitive modifier use with examples |
| NCCI Edit | Coding edit that blocks improper code combinations | Common reason beginners overbill or unbundle | Always check edit rationale before overriding |
| Charge Capture | Ensuring performed services become billable charges | Missed charges create silent revenue leakage | Compare documentation, orders, and billed services |
| EHR Workflow | How documentation moves through the electronic record | Coders fail when they cannot locate support efficiently | Learn where key elements live in each chart type |
| Encoder | Software that assists code selection and validation | Helpful tool, dangerous crutch | Use software to confirm logic, not replace logic |
| Compliance | Adherence to coding, billing, and regulatory rules | Trainees can create liability before they create value | Treat every shortcut as a future audit problem |
| PHI | Protected health information | Training settings still require full privacy discipline | Follow minimum-necessary access rules at all times |
| Competency Assessment | Formal evaluation of trainee skill readiness | Determines progression to harder charts or independent coding | Ask what skills are tested and how often |
| Remediation | Corrective training after repeated errors | Can rescue a trainee or expose weak instruction | Target one error cluster at a time |
| Specialty Rotation | Exposure to different departments or service lines | Builds range and reveals specialty-specific risk | Keep a separate reference sheet per specialty |
| Abstracting | Pulling required data elements from the chart | Weak abstracting leads to wrong coding downstream | Extract diagnoses, procedures, dates, and supporting facts systematically |
| Reconciliation | Matching coded output, charges, and payment outcomes | Connects coding choices to revenue reality | Review what got paid, reduced, or denied |
| Conversion Offer | Internship or apprenticeship leading to permanent role | Top goal for many trainees | Ask what benchmarks trigger hiring consideration |
2. Core apprenticeship structure terms every future coder must understand
The first group of terms defines how the training program itself works. If you misunderstand these, you can spend months in a program and still come out underprepared. Start with the difference between exposure and skill transfer. Shadowing gives visibility into coder thought processes, but competency comes from reviewed production, dual coding, and structured correction. That is why serious trainees study complete reference for coding query process terms, clinical documentation improvement CDI terms dictionary, guide to electronic medical records EMR documentation terms, and electronic health record EHR coding terms dictionary alongside specialty coding content.
A preceptor is not just a person who “checks your work.” A strong preceptor translates chart facts into code logic, explains why one sequencing choice is defensible and another is fragile, and helps you understand where software support ends. That is where complete reference for encoder software terms, guide to revenue cycle management software terms, medical billing practice management systems terms defined, and understanding medical coding automation terms become important. New coders who trust software too early often create clean-looking but weakly supported claims.
Competency assessment is another term that many beginners underestimate. A good assessment does not merely score whether you selected the “right code.” It tests abstracting discipline, record navigation, sequencing logic, modifier usage, documentation sufficiency recognition, escalation judgment, and consistency under time pressure. That is why programs with real value usually connect training to understanding coding edits modifiers complete guide, CPT modifiers dictionary usage and examples explained, comprehensive guide to CMS-1500 form terms and definitions, and UB-04 CMS-1450 billing form guide and terms explained, because real coding competency affects downstream billing artifacts.
Remediation is also not a bad sign by itself. In strong programs, remediation identifies exact error families: unsupported diagnoses, missed secondary conditions, misuse of modifiers, failure to detect medical necessity issues, or inconsistent abstracting. Trainees improve fastest when remediation is anchored in guide to professional development terms in medical coding, understanding continuing education units CEUs for coders, medical coding education accreditation terms, and complete guide to coding credentialing organizations, because long-term success depends on learning how to keep improving after formal training ends.
3. Documentation, compliance, and workflow terms that make or break trainees
Most apprenticeship breakdowns happen here. Beginners often think coding errors come from weak memory. In reality, many failures start with weak chart reading. A trainee may know the code book well and still miss the real principal diagnosis, overlook documentation contradictions, or fail to recognize when the record does not support the billed level. That is why comprehensive guide to SOAP notes and coding, comprehensive guide to problem lists in medical documentation, medicare documentation requirements for coders, and medical record retention and storage terms matter inside training, not just after hiring.
Compliance terms also hit beginners harder than expected because early habits become permanent habits. Guessing when documentation is vague, copying prior logic without rechecking current chart facts, or using a modifier to “make the claim go through” are not productivity tricks. They are risk behaviors. Strong apprenticeships teach trainees to think through guide to medical coding regulatory compliance, complete guide to coding ethics and standards, understanding Stark Law and Anti-Kickback Statute terms, and understanding medical coding system updates and releases as operating rules, not academic topics.
Workflow language matters just as much. You cannot become productive if you do not understand where information resides, how charges enter the system, when claims scrubbers fire, and where edits stop claims from moving. That is why practical trainees spend time with clearinghouse terminology guide for medical coders, guide to electronic data interchange EDI billing terms, guide to payment posting in medical billing, and medical billing reconciliation terms comprehensive guide. Once you see how the whole system moves, your code choices become more deliberate.
Even your note-taking system during training matters. Build a living reference around healthcare billing acronyms comprehensive dictionary and examples, medical abbreviations and acronyms dictionary for coders, reference understanding Medicare reimbursement fully, and commercial insurance billing terms essential guide. That habit helps you move from isolated memorization to pattern recognition, which is exactly what supervisors look for when deciding whether an intern is becoming dependable.
4. Revenue cycle, reimbursement, and analytics terms trainees must connect to their coding decisions
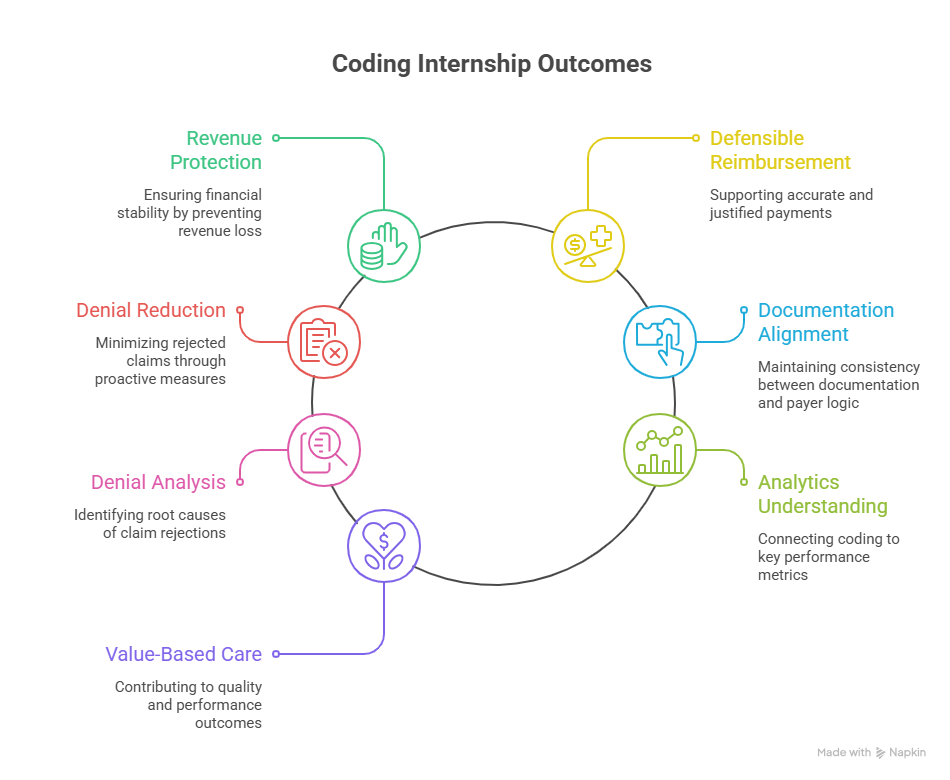
A weak internship teaches you how to assign codes. A strong internship teaches you what those codes do after submission. That difference matters because employers do not hire coders merely to finish charts. They hire coders to protect revenue, support defensible reimbursement, reduce preventable denials, and keep documentation aligned with payer logic. That is why trainees should study guide to medical coding revenue leakage prevention, comprehensive guide to charge capture terms, advanced guide to claims reconciliation terms, and understanding collections and bad debt in medical billing early.
Denial thinking should be part of apprenticeship training from day one. When trainees see a rejected or reduced claim, they should learn to ask: was the problem documentation support, modifier usage, medical necessity, coordination of benefits, payer policy mismatch, or demographic/claim form error? That mindset becomes sharper when paired with explanation of benefits EOB comprehensive guide, understanding coordination of benefits COB clear definitions, dictionary patient responsibility and copay terms clarified, and guide to healthcare claims management terms. Trainees who can interpret payment outcomes become far more valuable than trainees who only know isolated coding rules.
Analytics terms matter here too. Departments increasingly expect coders to understand why certain metrics are being tracked and what those metrics reveal. A beginner who can connect coding behavior to clean claim rate, edit rate, denial rate, touch count, lag days, and reimbursement variance stands out quickly. That is where guide to data analytics and reporting terms for coders, revenue cycle metrics and KPIs terms and definitions, understanding cost reporting in medical billing, and guide to physician fee schedule terms become career accelerators.
Value-based language is also no longer optional. Even trainees focused on basic coding should understand how documentation and coded data feed broader models through value-based care coding terms explained, Medicare Access and CHIP Reauthorization Act MACRA terms, comprehensive guide to Merit-Based Incentive Payment System MIPS, and comprehensive guide to risk adjustment coding. That knowledge helps trainees understand why precise documentation support is not just about one claim. It shapes quality scores, financial performance, and provider profiling.
5. How to evaluate an apprenticeship or internship and turn it into a full-time coding job
Not every internship deserves your time. Some are little more than observation, generic modules, and vague feedback. A serious pathway should show you what charts you will code, who will review your work, how quality will be measured, how feedback will be delivered, and what progression milestones unlock more independence. Before joining, evaluate the program against CBCS Certified Billing and Coding Specialist exam terms explained, online resources and communities for medical coding exam prep, understanding certification renewal and recertification terms, and guide to professional development terms in medical coding so your training strengthens long-term career value.
Ask targeted questions. What specialties are included? Are cases retrospective, concurrent, outpatient, professional fee, facility, or mixed? Will you work inside live or simulated electronic health record EHR coding terms dictionary workflows? Are trainees taught guide to utilization review and management terms for coders, hierarchical condition categories HCCs coding definitions, guide to healthcare effectiveness data and information set HEDIS, and accountable care organization ACO billing terms only as theory, or within actual coding decisions? The answer tells you whether the program is modern or outdated.
To convert training into a job offer, think like a low-risk hire. Build a measurable record of your growth. Keep a spreadsheet of chart types coded, error categories corrected, audit scores by month, denial-related lessons learned, specialties touched, and workflow systems used. Tie your improvements to guide to payment posting in medical billing, medical billing reconciliation terms comprehensive guide, guide to accurate medical billing and reimbursement, and revenue cycle management RCM terms explained. Hiring managers respond to evidence that your coding decisions are becoming cleaner, safer, and more operationally useful.
Finally, do not present yourself as “entry level but passionate.” Present yourself as a trainee who understands documentation integrity, escalation discipline, claim impact, payer sensitivity, workflow systems, and quality measurement. That message becomes credible when it is grounded in the language of medical coding workflow terms complete reference, medical coding audit terms comprehensive dictionary, guide to medical coding regulatory compliance, and coding competency and assessment terms defined. That is the profile employers trust.
6. FAQs
-
An apprenticeship is usually more structured, longer, and tied to progressive skill development under supervision. An internship may be shorter and can range from hands-on coding to mostly observational exposure. The better question is whether the program includes reviewed case work, measurable quality scoring, workflow exposure, and practical use of concepts from medical coding certification terms dictionary, medical coding workflow terms complete reference, guide to coding career development essential terms, and coding competency and assessment terms defined.
-
Look for live or realistic chart exposure, regular preceptor feedback, dual coding or chart comparison, documented remediation, specialty-specific cases, productivity expectations that scale responsibly, and clear conversion criteria for employment. A valuable program should expose you to guide to electronic medical records EMR documentation terms, complete reference for coding query process terms, understanding coding edits modifiers complete guide, and guide to medical coding regulatory compliance, not just general lectures.
-
Yes. Good programs expect low speed early. What matters first is abstracting discipline, documentation reading, code logic, escalation judgment, and correction uptake. Speed built on weak logic becomes a liability. Use the training period to strengthen fundamentals through clinical documentation improvement CDI terms dictionary, medical necessity criteria essential coding guide, guide to accurate medical billing and reimbursement, and medical coding audit terms comprehensive dictionary.
-
Document your chart volume, chart types, specialties, audit scores, error trends, remediation improvements, software exposure, and revenue-cycle understanding. Translate your experience into employer language by referencing guide to data analytics and reporting terms for coders, revenue cycle metrics and KPIs terms and definitions, guide to healthcare claims management terms, and guide to medical coding revenue leakage prevention. Employers trust evidence, not broad enthusiasm.
-
Start with documentation sufficiency, abstracting, principal diagnosis logic, modifier use, medical necessity, edits, query triggers, denial basics, productivity versus accuracy, and compliance boundaries. Those concepts unlock most of the work you will face first. Build outward from medical abbreviations and acronyms dictionary for coders, healthcare billing acronyms comprehensive dictionary and examples, clearinghouse terminology guide for medical coders, and guide to electronic data interchange EDI billing terms, because operational fluency reduces confusion fast.
-
Absolutely. One of the biggest hidden benefits of internships is discovering which documentation styles and coding logic fit your strengths. Exposure to specialties through resources such as guide to lab and pathology coding essentials, radiology billing and coding terms dictionary, telemedicine coding terms and definitions explained, and behavioral health billing terms comprehensive dictionary can reveal whether you prefer highly procedural environments, documentation-heavy specialties, recurring chronic-care logic, or payer-sensitive service lines.