
Medical Billing and Coding Certification in Hong Kong: Complete Guide for 2026-2027
Hong Kong is a serious healthcare market for anyone who wants medical billing and coding skills that travel across clinics, hospitals, insurers, outsourced billing teams, and remote revenue-cycle roles. A strong certification path should help you connect medical coding workflow terms, revenue cycle management terms, accurate billing and reimbursement, health information management terms, and medical coding certification terms into job-ready judgment.

1. Why Medical Billing and Coding Certification Matters in Hong Kong in 2026-2027
Hong Kong’s healthcare environment rewards people who understand documentation, coding logic, payer expectations, data privacy, and billing accuracy as one connected discipline. Public hospitals, private providers, insurance-backed care, specialist clinics, international patients, and remote billing teams all create pressure for clean records and reliable revenue-cycle work. A learner who studies clinical documentation improvement, medical necessity criteria, claim adjustment reason codes, remittance advice remark codes, and payment posting terms can understand the real life of a claim after code selection.
Certification matters because Hong Kong learners may pursue several career directions. Some want private clinic billing roles. Some want hospital documentation or health-information roles. Some want insurer, TPA, or claims-administration work. Some want remote U.S.-style coding and billing roles where CPT, ICD, HCPCS, modifiers, EOBs, and payer edits matter heavily. That is why a smart study plan should include CPT modifiers, coding edits, commercial insurance billing, coordination of benefits, and healthcare data security.
The strongest candidates think beyond passing an exam. They can read a chart, identify missing specificity, assign defensible codes, check claim form logic, interpret payer responses, correct denials, protect patient data, and explain revenue leakage. Hong Kong’s mix of advanced digital health systems, private insurance use, specialist care, and cross-border healthcare expectations makes this practical skill especially valuable. Build your foundation with charge capture terms, revenue leakage prevention, claims management terms, claims reconciliation, and revenue cycle KPIs before trusting any training path.
Hong Kong Certification Roadmap: 30 Skills That Actually Matter
| Skill Area | What It Means | Why It Matters in Hong Kong | Best Practice Action |
|---|---|---|---|
| Coding workflow | How documentation becomes coded, billed, reviewed, and paid | Hong Kong learners need a full claim-path view, especially for private and insurer-linked workflows | Map every case from patient encounter to final payment outcome |
| HIM basics | Health record governance, documentation quality, and information control | Digital health records require disciplined record handling and access awareness | Learn record ownership, privacy, retention, and audit trail basics |
| CDI | Improving provider documentation before final coding | Vague notes create coding risk, payer friction, and weak claim support | Query missing laterality, severity, timing, procedure detail, and diagnosis support |
| Medical necessity | The link between patient condition and billed service | Insurer-backed claims fail when the note does not justify the service | Tie every procedure to symptoms, diagnosis, test results, or clinical rationale |
| Modifier logic | Coding signals that explain service circumstances | Remote U.S.-style coding and specialty billing often depend on correct modifier use | Build examples for bilateral, distinct, repeat, and professional/technical billing scenarios |
| Coding edits | Rules that catch incompatible, bundled, or unsupported code combinations | Edit knowledge helps learners prevent rejections before payer review | Review edit logic before submitting or appealing questionable code pairs |
| Charge capture | Capturing all billable services from the clinical encounter | Private clinics lose money when performed services never reach the claim | Compare orders, notes, procedure logs, supplies, and final charges |
| Revenue leakage | Lost revenue from missed charges, undercoding, denials, and underpayments | High-cost city healthcare operations need tight revenue discipline | Track repeated leakage by specialty, provider, payer, and code family |
| EOB review | Reading payer payment, adjustment, denial, and patient balance details | EOB skill separates practical billing candidates from code-only learners | Summarize each EOB by billed amount, allowed amount, paid amount, adjustment, and next action |
| CARCs | Standard reason codes explaining claim adjustments | They help billing teams identify denial causes quickly | Create a denial-response sheet for recurring adjustment reasons |
| RARCs | Remark codes that add detail to payer decisions | They expose documentation gaps, submission issues, and correction needs | Pair RARCs with CARCs before correcting or appealing claims |
| Commercial insurance | Private payer plans, coverage logic, and reimbursement rules | Hong Kong private care often interacts with insurance-backed payment expectations | Study eligibility, policy limits, preauthorization, exclusions, and reimbursement language |
| COB | Determining payment order when more than one plan exists | International workers and family coverage can create payment-order confusion | Verify primary payer, secondary payer, patient responsibility, and documentation proof |
| Clearinghouse checks | Electronic claim validation before payer acceptance | Remote billing workflows often depend on fast rejection correction | Separate technical rejections from payer denials during follow-up |
| EDI billing | Electronic exchange of claim, remittance, and eligibility data | Cross-system billing requires clean data transfer and field accuracy | Learn basic claim file, remittance, and eligibility transaction language |
| CMS-1500 | Professional claim form structure for outpatient and physician billing | Remote U.S.-style billing roles often expect claim form familiarity | Practice provider, diagnosis, procedure, modifier, charge, and payer field placement |
| UB-04 | Institutional claim form structure | Hospital-linked billing requires facility claim awareness | Study revenue codes, bill types, occurrence codes, value codes, and discharge status |
| Payment posting | Applying insurer and patient payments to accounts | Posting errors hide underpayments, false balances, and appeal opportunities | Match expected allowed amounts against actual payer decisions |
| Reconciliation | Matching billed, allowed, paid, adjusted, denied, and outstanding amounts | It turns billing from guesswork into measurable account control | Reconcile by payer, date of service, denial reason, and aging bucket |
| Coding audits | Checking coded cases for documentation support and compliance risk | Audit discipline builds employer trust faster than vocabulary alone | Audit by provider, code family, modifier use, and denial outcome |
| Query process | Formal clarification when documentation lacks required detail | Coders must avoid assumptions when the record is unclear | Use neutral, compliant, evidence-based query language |
| EHR coding | Coding from electronic notes, templates, orders, and results | Electronic records can contain copy-forward errors and conflicting fields | Verify dates, provider signatures, clinical detail, and final assessment |
| EHR integration | How clinical, coding, billing, and payer systems connect | System mapping errors can break clean claims even when coding is accurate | Test provider, payer, diagnosis, procedure, charge, and claim-field mapping |
| Data security | Protecting patient information, billing data, and access permissions | Digital records and remote work demand strict privacy discipline | Use secure devices, role-based access awareness, and minimum necessary data habits |
| Encoder software | Tools that support code lookup and coding validation | Software helps only when the coder can verify the final decision | Treat software output as a prompt for review, documentation matching, and audit logic |
| Practice management systems | Billing platforms that manage schedules, claims, balances, and payments | Clinic billing depends on system accuracy as much as code accuracy | Learn appointment, charge, claim, payment, and aging workflows |
| Coding automation | Computer-assisted coding, AI support, and automated suggestions | Automation increases the value of coders who can audit output | Validate every suggestion against actual note evidence |
| Data analytics | Using reports to find denial, coding, payment, and productivity patterns | Advanced billing teams need people who can explain trends | Build reports for clean claim rate, denial rate, AR aging, and underpayment risk |
| CEUs | Ongoing learning after certification | Healthcare rules, payer logic, code sets, and software expectations keep changing | Plan annual education across coding, billing, compliance, and specialty updates |
2. What a Strong Certification Program Should Teach Hong Kong Learners
A serious certification program should begin with medical terminology, anatomy, documentation structure, diagnosis coding, procedure coding, modifier use, claim forms, denial language, compliance, privacy, and audit evidence. Hong Kong learners should avoid courses that teach isolated code lookup without chart interpretation. Real work starts when the note has missing laterality, the provider selected a vague diagnosis, the payer questions medical necessity, or the claim fails a system edit. Strengthen the base with medical abbreviations for coders, SOAP notes and coding, problem list documentation, EMR documentation terms, and clinical decision support terms.
The next layer is specialty coding. Hong Kong has a dense specialist healthcare market, so learners should practice beyond basic office visits. A billing or coding candidate who understands radiology, cardiology, dermatology, gastroenterology, emergency medicine, pathology, telemedicine, and preventive care becomes more useful to employers. Use AMBCI’s guides for cardiology CPT coding, radiology procedures, emergency medicine codes, gastroenterology procedures, and dermatology coding to build practical range.
The third layer is payer behavior. Many beginners can assign a code during study, then freeze when an EOB, rejection, adjustment, authorization issue, patient balance, or appeal arrives. Hong Kong learners who want private clinic, insurer, TPA, or remote billing work need payer literacy from the start. Study commercial insurance billing, patient responsibility terms, collections and bad debt, utilization review terms, and claims reconciliation so your certificate is backed by real workflow judgment.
3. How to Choose the Right Certification Path in Hong Kong
Choose the certification path based on the role you want. For clinic billing, prioritize eligibility, registration accuracy, charge capture, claim submission, payment posting, patient balances, and denial follow-up. For coding-heavy roles, prioritize anatomy, documentation, diagnosis specificity, CPT or procedure logic, modifiers, compliance, and audit defense. For insurer or claims-administration work, prioritize policy terms, documentation requirements, preauthorization, adjudication language, EOB review, and appeals. Compare credentialing organization terms, medical coding education accreditation, CBCS exam terms, coding competency assessment, and certification renewal terms.
If your target is remote international coding, be extra careful. Remote jobs often expect proof that you can work independently, follow payer-specific rules, protect data, handle productivity expectations, and explain your coding rationale. A certificate helps, but employers trust examples. Build sample work around CMS-1500 claim terms, UB-04 institutional billing, clearinghouse terminology, EDI billing terms, and RCM software terms so you sound operational, not theoretical.
A strong course should give learners practice cases, feedback, denial examples, claim form training, privacy rules, coding scenarios, audit exercises, and career guidance. Weak programs overload learners with definitions and leave them unable to solve payer problems. Before paying, ask whether the course includes real-case documentation, specialty coding, EOB interpretation, modifier scenarios, and compliance-based review. Use online CPC certification program directories, CBCS certification course directories, CCS certification program directories, coding career development terms, and professional development terms to judge long-term value.
Quick Poll: What is your biggest medical billing and coding certification fear in Hong Kong?
4. Step-by-Step Plan to Become Job-Ready in Hong Kong
Start with the language of healthcare records. A learner who cannot understand patient history, assessment language, orders, operative notes, diagnostic reports, medication references, and follow-up plans will struggle with coding accuracy. Spend your first stage on documentation structure, medical abbreviations, anatomy, disease terminology, and provider note logic. Build that foundation with medical abbreviations, health information management, EMR documentation terms, problem list documentation, and medical record retention before heavy code practice.
Then build your diagnosis and procedure coding muscle. Practice across common conditions, chronic disease, imaging, labs, emergency visits, outpatient procedures, and specialty services. Hong Kong learners targeting remote work should also become comfortable with U.S.-style procedure and payer language. Use ICD-11 cardiovascular coding, ICD-11 oncology reference, ICD-11 infectious disease coding, lab and pathology coding, and preventive medicine CPT coding to practice breadth.
After coding practice, move into the revenue-cycle layer. Learn what happens when a claim is created, edited, submitted, rejected, adjudicated, paid, adjusted, appealed, or sent to patient responsibility. This is the layer that exposes weak training. A coder who cannot explain why a claim failed will lose employer confidence fast. Study claims management terms, denial management services, payment posting, medical billing reconciliation, and directory of electronic claim submission platforms to understand the work after submission.
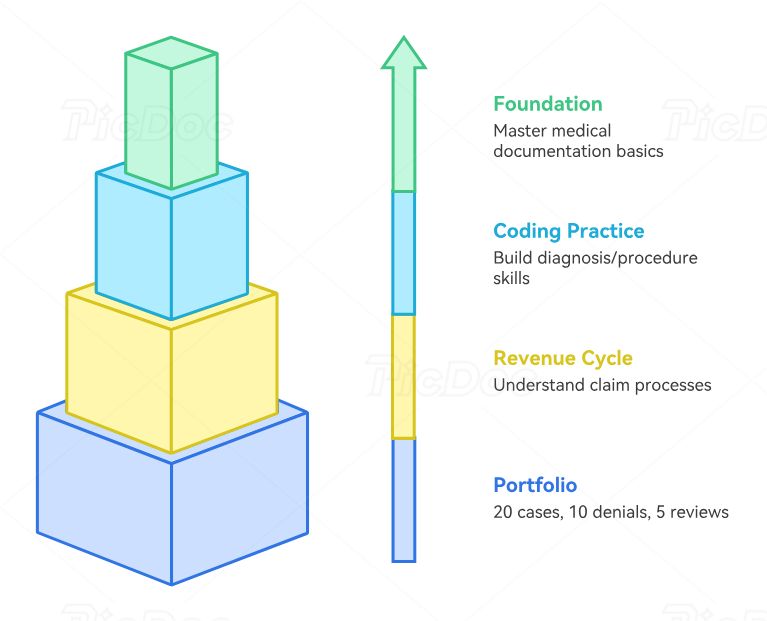
Finish by creating a proof-based portfolio. Include 20 coded case summaries, 10 denial breakdowns, 5 modifier explanations, 5 medical necessity reviews, 5 EOB interpretations, 3 claim correction examples, and 3 audit worksheets. Each example should show the chart issue, your decision, the code or billing logic, the risk, and the corrective action. Use medical coding audit terms, coding query process terms, data analytics for coders, revenue cycle metrics, and coding competency assessment to make your portfolio practical.
5. Common Mistakes Hong Kong Learners Should Avoid Before Certification
The first mistake is choosing a program before choosing a career direction. A clinic billing assistant, a claims analyst, a hospital coding trainee, a remote U.S. medical coder, and a revenue-cycle analyst need different strengths. A certificate can support any of those paths, but the study plan must match the job target. Use coding career development terms, medical coding apprenticeship terms, professional development terms, coding competency assessment, and continuing education units to plan skill growth with purpose.
The second mistake is ignoring documentation quality. Codes depend on what the record supports. When the diagnosis is vague, the procedure note lacks detail, the assessment conflicts with the plan, or the order does not support the billed service, the claim becomes vulnerable. Strong learners practice asking what the record proves. Train with CDI terms, medical necessity guidance, coding query process terms, utilization review terms, and clinical decision support terms.
The third mistake is treating software as a shortcut. EHRs, encoder tools, practice management systems, clearinghouses, AI suggestions, dashboards, and payer portals can help, but they can also hide errors. A smart learner can explain where the system might break: wrong provider mapping, wrong payer selection, missing authorization, invalid modifier, copied documentation, failed edit, underposted payment, or aging account silence. Strengthen that system awareness with encoder software terms, practice management systems, RCM software terms, coding automation, and EHR integration.
The fourth mistake is leaving interview preparation until the week before applying. Start building interview answers while you study. Practice explaining how you handle missing documentation, why medical necessity matters, how you respond to denials, how you read an EOB, how you protect patient data, how you catch underpayments, and how you keep learning after certification. Build answers using EOB guidance, CARCs, RARCs, healthcare data security, and coding ethics.
6. FAQs About Medical Billing and Coding Certification in Hong Kong
-
Yes, it can be useful when it proves practical coding, documentation, billing, and payer-workflow competence. Hong Kong learners should treat certification as a structured proof of ability, then support it with case practice, EOB review, denial analysis, and audit examples. A strong learner should understand medical coding certification terms, medical coding workflow, accurate reimbursement, RCM terms, and billing acronyms.
-
Choose based on the role you want. Coding-focused learners should prioritize diagnosis coding, procedure coding, medical necessity, modifiers, documentation, and audits. Billing-focused learners should prioritize claims, payer terms, EOBs, payment posting, patient balances, and denials. Compare CBCS exam terms, credentialing organizations, online CPC certification programs, CCS certification programs, and coding education terms.
-
Remote opportunities are possible when learners can prove accuracy, privacy discipline, payer literacy, software comfort, and independent workflow control. Remote employers often expect clear written communication, dependable productivity, denial follow-up awareness, and strong documentation judgment. Build remote readiness with healthcare data security, EHR coding terms, claim management terms, coding automation terms, and data analytics reporting.
-
A focused learner can build beginner readiness in a few months, while stronger job readiness requires case practice, specialty coding, denial work, billing workflow exposure, and portfolio building. The timeline depends on healthcare background, English documentation comfort, weekly study hours, and practice quality. Use medical terminology resources, ICD-11 coding standards, CPT modifier examples, EOB interpretation, and coding audits to speed up practical learning.
-
A strong portfolio should include coded sample cases, diagnosis-to-procedure support, modifier examples, denial explanations, EOB breakdowns, medical necessity checks, claim correction examples, and mini-audit worksheets. Each example should explain the documentation, coding decision, billing risk, and corrective action. Use medical necessity criteria, charge capture terms, revenue leakage prevention, claims reconciliation, and coding competency assessment as your framework.
-
The biggest mistake is choosing a course because it sounds official while ignoring practice depth. A valuable course should teach documentation, coding, billing, denials, claim forms, payer language, compliance, and audit proof. Before enrolling, compare the curriculum with actual job duties. Review medical coding education accreditation, coding credentialing organizations, coding career development, professional development terms, and certification renewal terms.
-
Plan continuing education from the start. Coding rules, payer policies, documentation expectations, software workflows, privacy requirements, and specialty billing rules change over time. Review denial patterns, audit findings, coding updates, payer notices, and CEU options regularly. Keep studying CEU requirements, medical coding system updates, ICD-11 best practices, revenue cycle KPIs, and coding competency assessment so your certification stays current.