
Medical Billing and Coding Certification in South Korea: Complete Guide for 2026–2027
Medical billing and coding in South Korea requires a precise understanding of Korean clinical terminology, national insurance rules, KCD diagnosis classification, HIRA claim review, hospital information systems, and medical-record governance. Candidates must also separate a short professional certificate from South Korea’s regulated Health Information Manager licensing route. This guide explains the available pathways while connecting them with medical coding workflows, healthcare claims management, revenue-cycle operations, and coding compliance for 2026–2027.

1. Understanding Medical Billing and Coding Careers in South Korea
South Korea’s reimbursement environment revolves heavily around National Health Insurance. The National Health Insurance Service administers the insurance program, while the Health Insurance Review and Assessment Service reviews benefit claims, evaluates healthcare quality, and supports the management of reimbursement standards. Healthcare providers submit claim statements containing services and costs, after which claims can pass through electronic checks, professional review, post-management, or appeal processes.
This structure shapes the work performed by Korean billing, claims, and health-information professionals. A hospital employee may need to validate patient eligibility, confirm whether a service is covered, apply the correct diagnosis and procedure classifications, reconcile medication and supply data, investigate a reduction made during review, prepare supporting documentation, and monitor eventual payment. These activities draw on billing and reimbursement knowledge, medical necessity review, charge-capture controls, and claims reconciliation.
The most important distinction for candidates concerns credential type. South Korea has a licensed profession called Health Information Manager, or 보건의료정보관리사. Obtaining this license requires graduation from an accredited university program, completion of prescribed subjects, passing the national examination, and receiving a license from the Minister of Health and Welfare. A short online billing certificate cannot replace this route when an employer specifically requires the national license.
Health Information Management is broader than claim entry. It can include clinical data collection, disease classification, medical-record quality, statistical reporting, cancer registration, privacy, information release, coding quality, data analysis, reimbursement support, and electronic-record governance. Candidates comparing this profession with narrower billing work should study the health information management terms, electronic medical-record concepts, clinical documentation improvement, and healthcare data-security requirements attached to the role.
A separate Korean qualification pathway focuses more directly on insurance review and claims management. The Korean Health Information Management Association has operated an Insurance Review Claims Manager examination assessing health-insurance theory, benefit standards, automobile and industrial-accident insurance, medical-aid rules, long-term-care hospital payment standards, and practical claim review. Its published eligibility conditions include students or graduates of accredited Health Information Management programs who completed relevant coursework, as well as licensed Health Information Managers with specified professional experience.
This means candidates should verify eligibility before paying for preparation. A course may teach useful insurance billing terminology, payment-posting processes, account-audit methods, and revenue-cycle metrics, yet completion of that course does not automatically establish eligibility for a regulated or association-administered examination.
The classification environment also changed for 2026. Statistics Korea announced that the ninth revision of the Korean Standard Classification of Diseases and Causes of Death, KCD-9, would take effect on January 1, 2026. The revision retains the ICD-10-based structure while incorporating international updates and changes relevant to Korea’s healthcare environment. Anyone studying from older KCD-8 books, practice cases, or software screenshots must check whether the material has been updated.
KCD accuracy affects much more than code memorization. Diagnosis classification can influence claim review, disease statistics, quality measurement, severity analysis, research data, registries, and documentation queries. A credible curriculum should therefore connect coding-system updates, medical coding automation, encoder-software controls, and coding competency assessment with KCD-9 implementation.
South Korea Certification Competency Map: 30 Skills Employers Can Test
| Competency | What You Must Understand | Risk It Controls | Portfolio Evidence |
|---|---|---|---|
| Korean healthcare structure | Roles of MOHW, NHIS, HIRA, medical institutions, private insurers, and other payers | Sending an account through the wrong reimbursement workflow | Create a one-page payer and regulator map |
| NHIS coverage | Insured benefits, patient cost sharing, eligibility, coverage limitations, and payment responsibility | Incorrect patient balances and coverage assumptions | Complete ten benefit-verification cases |
| HIRA claim review | Electronic checks, professional review, supporting evidence, reductions, objections, and post-management | Unresolved claim reductions and repeated review failures | Map a complete claim-review workflow |
| KCD-9 | Classification structure, inclusion rules, exclusions, sequencing, specificity, and 2026 revisions | Outdated or unsupported diagnosis assignment | Code 30 de-identified diagnosis cases |
| Clinical terminology | Korean and English anatomy, pathology, treatments, abbreviations, and diagnostic language | Misreading the record or overlooking a key condition | Build a bilingual specialty glossary |
| Clinical documentation | Dates, signatures, provider intent, procedure detail, chronology, contradictions, and amendments | Submitting charges without defensible record support | Perform a documentation audit |
| Principal diagnosis | Reason for admission, confirmed conditions, sequencing, complications, and comorbidities | Incorrect inpatient classification and data distortion | Write ten sequencing rationales |
| Secondary diagnoses | Conditions affecting care, monitoring, treatment, evaluation, or resource use | Missing severity data or reporting irrelevant conditions | Audit 15 inpatient records |
| Procedure classification | Service selection, operative detail, approach, site, quantity, date, and documentation support | Payment reduction and procedure mismatches | Complete a procedure-validation worksheet |
| Fee-schedule interpretation | Covered services, units, conditions, restrictions, combinations, and effective dates | Overcharging, undercharging, and invalid combinations | Annotate a simulated fee schedule |
| Benefit standards | Clinical and administrative conditions required for reimbursement | Claims failing despite a correctly selected code | Build a medical-necessity checklist |
| Patient registration | Identity, eligibility, referral information, demographics, payer data, and encounter details | Front-end denials and incorrect patient attribution | Create a registration quality checklist |
| Referral verification | When referral documents or institutional pathways affect access and reimbursement | Coverage disputes and invalid tertiary-care claims | Design a referral exception log |
| Charge capture | How procedures, drugs, supplies, imaging, rooms, and professional work reach the account | Revenue leakage and duplicate billing | Complete a charge reconciliation |
| Drug billing | Product identification, route, dose, quantity, waste, coverage rules, and administration evidence | Unit errors and unsupported medication charges | Audit ten medication cases |
| Supply and device billing | Item identity, traceability, quantity, procedure linkage, approval status, and documentation | High-value supply reductions and duplicate charging | Build a device traceability worksheet |
| Claim editing | Duplicate detection, incompatible services, missing fields, invalid dates, and logic conflicts | Preventable electronic rejections | Create an edit-resolution guide |
| Claim submission | Required data, electronic transmission, acceptance, rejection, correction, and tracking | Claims disappearing between systems | Draw an end-to-end submission map |
| Reduction analysis | Review decision, financial amount, root cause, corrective action, deadline, and recurrence | Permanent loss of recoverable revenue | Build a reduction root-cause dashboard |
| Appeals and objections | Supporting records, clinical rationale, benefit rule, filing period, and status monitoring | Weak appeals and missed recovery deadlines | Write five evidence-based appeal cases |
| Payment reconciliation | Claimed, reviewed, approved, reduced, paid, adjusted, and outstanding amounts | Hidden underpayments and inaccurate receivables | Complete a payment reconciliation |
| Accounts receivable | Aging, expected reimbursement, pending review, appeal status, and follow-up priority | Cash delays and forgotten claims | Segment an aging report by action |
| DRG awareness | Case grouping, included services, outliers, quality impact, and documentation sensitivity | Incorrect assumptions about separately billable services | Compare itemized and case-based payment |
| Quality assessment | Data completeness, indicators, credibility checks, provider comparison, and improvement action | Poor-quality submissions and unreliable performance results | Create a quality-data validation sheet |
| Electronic medical records | Templates, authentication, amendments, interfaces, structured fields, and audit trails | Missing evidence and inaccurate data transfer | Map an EHR integration workflow |
| Personal information protection | Sensitive data, authorized use, access limitation, retention, safeguards, and breach response | Unauthorized disclosure of medical information | Design a role-based access matrix |
| Record retention | Storage, retrieval, amendment, release, legal holds, destruction, and audit evidence | Missing documentation during review or litigation | Create a retention schedule |
| Spreadsheet analytics | Lookups, pivots, duplicate detection, exception flags, aging, and trend analysis | Slow investigations and unnoticed patterns | Build an interactive claim-error workbook |
| Revenue-cycle KPIs | Clean-claim rate, reduction rate, rework, recovery, aging, productivity, and error recurrence | Measuring activity without measuring results | Create a monthly KPI dashboard |
| Continuing education | KCD revisions, HIRA criteria, payment updates, privacy rules, system edits, and audit findings | Certified knowledge becoming operationally obsolete | Write a 12-month learning plan |
2. Choosing the Right Certification Path for Your Career Goal
A South Korean candidate should choose a credential according to the role’s legal status, employer expectations, reimbursement system, and working language. The title “medical billing and coding certification” can refer to several very different outcomes. One program may prepare students for domestic hospital claims, another may support a regulated Health Information Manager pathway, and another may teach U.S. coding for overseas clients.
The licensed Health Information Manager pathway
This is the strongest domestic route for candidates who want professional responsibility across medical records, disease classification, health statistics, information governance, and clinical data quality. The official pathway requires an accredited university program covering the prescribed curriculum, followed by the national examination and ministerial licensing.
Because this is a university-based licensing route, candidates should verify the institution’s current accreditation before enrollment. The decision should include curriculum quality, practical placement, KCD training, examination preparation, hospital partnerships, faculty expertise, and graduate employment. Useful supporting study areas include HIM terminology, medical coding education standards, clinical documentation, and professional coding ethics.
Foreign degree holders should avoid assuming that an overseas diploma automatically creates examination eligibility. Eligibility depends on South Korean legal and examination requirements, program recognition, subject completion, and document review. The safest action is to request a written eligibility determination from the responsible examination or licensing body before purchasing exam preparation.
The insurance review and claims route
This pathway suits professionals focused on reimbursement rules, claims preparation, HIRA review, reductions, objections, benefit standards, account auditing, and payment follow-up. The Insurance Review Claims Manager qualification described by the Korean association evaluates both theoretical and practical claim-review competencies, but its eligibility requirements restrict who can sit for the examination.
Students pursuing this route should master healthcare claims management, medical billing reconciliation, utilization review, and payment posting. A candidate who can enter a claim yet cannot explain a reduction, identify the controlling benefit standard, or assemble an appeal remains difficult to place in higher-responsibility work.
Short private certificates
Private training can help career changers learn terminology, claim flow, spreadsheets, documentation review, and basic account auditing. Its value depends on the curriculum, assessment quality, instructor experience, practical cases, and employer recognition. Candidates should ask whether the certificate teaches South Korean billing architecture or simply repackages U.S. material.
A high-value program should contain assessed cases involving registration, clinical records, KCD-9, fee schedules, HIRA review logic, corrections, payment reconciliation, privacy, and system updates. It should also connect billing practice-management systems, RCM software, coding audit concepts, and revenue-leakage prevention with Korean operational scenarios.
International coding credentials
CPC, CCS, CBCS, or similar credentials can support careers involving U.S. healthcare accounts, multinational RCM companies, research, education, or global coding projects. These credentials teach systems that differ from domestic Korean reimbursement. U.S.-facing work can require ICD-10-CM, CPT, HCPCS, CMS-1500, UB-04, NCCI edits, Medicare rules, commercial insurance, EOBs, CARCs, RARCs, and HIPAA-oriented processes.
Candidates should prepare through the CMS-1500 form guide, UB-04 billing reference, CPT modifier dictionary, and Medicare documentation guide. An international certificate supports the system named in its examination blueprint. It does not grant South Korea’s Health Information Manager license.
3. What a South Korea-Ready Curriculum Must Cover
The first requirement is bilingual clinical literacy. Domestic records, payer criteria, examination materials, and internal hospital communication are commonly handled in Korean. International medical terminology still matters because many disease names, procedures, drugs, devices, and classification references have English or Latin roots. Learners should be able to interpret Korean clinical narratives while recognizing standardized terminology used in medical abbreviations, electronic health records, problem lists, and SOAP notes.
KCD-9 deserves a dedicated module. Training should address code construction, chapter conventions, inclusion and exclusion instructions, symptom coding, confirmed diagnoses, suspected conditions, external causes, neoplasms, injuries, complications, and sequencing. Students should compare KCD-8 and KCD-9 changes rather than trusting old code lists. Statistics Korea’s decision to implement KCD-9 from January 2026 makes version control a direct competency for this article’s 2026–2027 audience.
Learners also benefit from understanding the direction of ICD-11 even while KCD remains ICD-10-based. Studying ICD-11 coding standards, ICD-11 mental-health classifications, neurological coding changes, and oncology coding case studies helps candidates understand future migration risks without mixing classifications in live work.
The curriculum must explain reimbursement logic from beginning to end. HIRA documentation describes a claims-review process beginning with provider submission, followed by electronic review, possible professional assessment, post-management, and opportunities for objection supported by evidence.
Students should therefore trace accounts through registration, eligibility, clinical documentation, charge capture, diagnosis coding, procedure reporting, fee calculation, claim editing, submission, review, payment, reduction investigation, objection, and final reconciliation. The RCM terms guide, claims-reconciliation reference, collections terminology, and revenue-cycle KPI dictionary help make that sequence measurable.
Medical-record quality should be assessed separately from code accuracy. A code may be technically valid while remaining unsupported because the record lacks a signed diagnosis, procedure detail, clinical indication, dosage, treatment duration, or required test result. Students should practise identifying incomplete, inconsistent, copied, or ambiguous documentation and drafting neutral clarification requests. The coding query guide, CDI dictionary, medical necessity reference, and coding compliance guide support this skill.
Privacy and medical-record governance also require serious treatment. South Korea’s Personal Information Protection Act establishes controls around sensitive information, limitations on processing, safeguards, privacy policies, breach notification, access, correction, erasure, and suspension of processing. Medical billing teams handle diagnostic, treatment, identification, and financial information, making privacy controls part of everyday competence.
Practical training should cover access limitation, secure transmission, minimum-necessary use, de-identification, storage, retention, screen privacy, printing, audit logs, incident escalation, and disposal. Candidates can reinforce these areas through healthcare data-security terms, medical-record retention, coding ethics, and EHR integration controls.
Quick Poll: What is blocking your medical coding career in South Korea?
4. Step-by-Step Certification Roadmap for 2026–2027
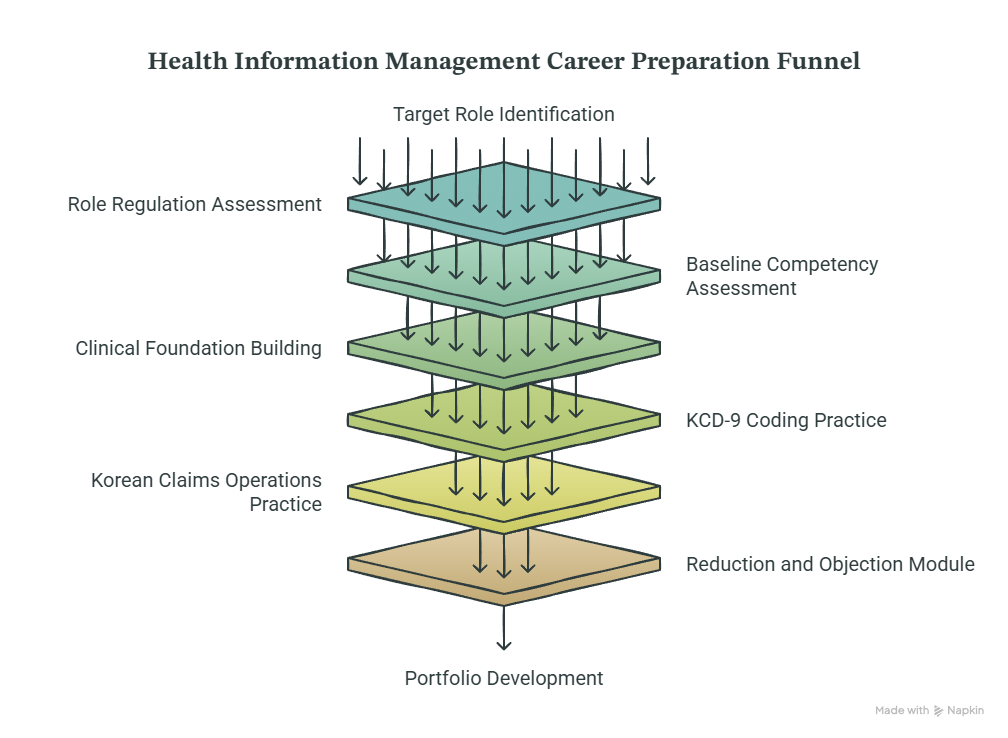
Begin by identifying one target role. Search for positions involving health information management, insurance review, claims examination, hospital administration, medical records, disease classification, clinical data, reimbursement, or international coding. Record each vacancy’s required degree, license, certification, experience, language, software, specialty, and reimbursement knowledge. This prevents a candidate from preparing for a respected credential that the intended employer never requests.
Next, determine whether the role is regulated. A vacancy requiring the Korean Health Information Manager license points toward the accredited university and national examination route. A claims-support position may accept healthcare administration, nursing, billing experience, or employer-specific training. An international role may prioritize CPC, CCS, CBCS, U.S. coding knowledge, and English communication. Compare options using the coding credentialing guide, certification terms dictionary, coding education terminology, and certification-renewal guide.
Complete a baseline assessment before studying. Test anatomy, terminology, KCD, documentation, spreadsheets, claim flow, privacy, and account reconciliation separately. A candidate who scores well in terminology may still struggle with payer logic. Someone with hospital experience may understand the workflow but repeatedly select nonspecific diagnoses. Use the competency-assessment guide, medical abbreviations dictionary, coding workflow reference, and HIM terminology guide to structure the assessment.
Build your foundation around medical language and documentation. Learn anatomy and disease processes by body system, then connect each diagnosis with common tests, treatments, procedures, medications, and record types. Read complete cases instead of isolated code descriptions. Introduce specialty references such as cardiology procedure coding, radiology terminology, laboratory coding, and surgical coding compliance according to your target department.
Move into KCD-9 only after building this clinical foundation. Code inpatient, outpatient, emergency, chronic-disease, oncology, injury, maternity, pediatric, psychiatric, and infectious-disease cases. For every answer, record the documentation phrase supporting the code, the classification instruction followed, the sequencing reason, and any clarification needed. This method develops defensible coding rather than pattern recognition.
The next phase should cover Korean claims operations. Follow an account from patient registration through HIRA review and payment. Practise finding missing identifiers, unsupported services, quantity errors, duplicate charges, outdated codes, inconsistent dates, absent benefit criteria, and incomplete records. Build exercises around charge capture, coding edits, claims management, and medical billing reconciliation.
Create a reduction and objection module. For each reduced service, record the amount, review reason, rule involved, documentation available, recoverability, deadline, corrective owner, objection status, and final financial result. This turns random follow-up into controlled denial management. International candidates can strengthen the same reasoning through CARC terminology, RARC definitions, coordination-of-benefits concepts, and EOB interpretation.
Your portfolio should contain a KCD-9 coding workbook, documentation audit, claim edit report, reduction root-cause dashboard, objection letter, payment reconciliation, and privacy risk assessment. Remove names, registration numbers, dates of birth, addresses, record numbers, and other identifying details. Synthetic cases are safer for public portfolios than altered real patient records.
Finish with timed practice and an error log. Divide errors into terminology gaps, documentation misinterpretation, classification mistakes, sequencing errors, outdated-reference use, benefit-rule confusion, calculation mistakes, and time pressure. Review the cause behind each wrong answer before completing another practice set. Support this stage with exam-preparation resources, career-development terms, professional-development planning, and continuing-education guidance.
5. Building a Competitive Career After Certification
Certification becomes valuable when it changes how you handle real records and claims. Employers need professionals who can protect data, interpret documentation, select the correct classification, detect billing defects, explain a review outcome, and close the financial loop. Your résumé should show these actions rather than listing course modules.
Use achievement-focused descriptions such as “audited simulated inpatient records for diagnosis-sequencing and documentation defects,” “built a KCD-9 change log for 2026 implementation,” or “created a claim-reduction dashboard separating coding, documentation, benefit-standard, and data-entry causes.” These statements demonstrate skills connected to coding audits, data analytics, revenue-leakage prevention, and claims reconciliation.
For domestic hospital roles, prepare to explain how you would investigate a reduced claim. Begin with the HIRA decision and financial amount. Verify patient and encounter information, dates, diagnosis, service, quantity, benefit standard, documentation, fee calculation, and system transmission. Identify whether the correction belongs to registration, the clinical department, coding, billing, pharmacy, materials management, or IT. End with an objection deadline, evidence list, responsible owner, resubmission status, and payment verification.
For Health Information Management roles, demonstrate broader data governance. Be ready to discuss record completeness, KCD classification, information release, registry quality, statistical accuracy, privacy, retention, EHR templates, and audit trails. Strengthen interview preparation through record-retention terminology, EHR integration concepts, clinical decision-support terms, and healthcare data security.
International candidates should build a separate résumé version. Emphasize ICD-10-CM, CPT, HCPCS, claim forms, modifiers, payer policies, EOBs, denials, English documentation, secure remote work, and destination-market compliance. Useful study areas include commercial insurance billing, Medicare reimbursement, physician fee schedules, and electronic claims submission.
Korean language ability can be decisive for domestic work because clinical records, review criteria, internal messages, and examination materials demand precise reading. General conversational fluency offers limited protection against misreading an abbreviation, hedged diagnosis, temporal statement, or benefit restriction. Build a specialty glossary and practise explaining each record in plain Korean before assigning codes.
Long-term progression can lead toward senior coding, insurance review, reimbursement management, clinical documentation improvement, medical-record administration, data quality, privacy, cancer registration, quality assessment, revenue integrity, analytics, training, or health-information systems. Choose the next competency according to the problem you repeatedly solve. Documentation defects point toward CDI. Recurrent reductions point toward benefit standards and claims review. Interface defects point toward data mapping and system integration.
6. Frequently Asked Questions About Certification in South Korea
-
South Korea uses several pathways. The regulated Health Information Manager profession requires an accredited university education, prescribed coursework, a national examination, and a license from the Minister of Health and Welfare. Claims-focused association qualifications and private certificates follow different eligibility and recognition rules.
Candidates should compare the role with the credentialing organization guide, certification dictionary, education accreditation terms, and renewal requirements before enrolling.
-
A short course does not replace the statutory pathway. The Korean association states that candidates must graduate from an accredited university program, complete prescribed subjects, pass the national examination, and obtain the ministerial license.
Online training can still strengthen medical terminology, coding workflows, claims management, and revenue-cycle skills, especially for support roles that do not require the national license.
-
Students targeting South Korean work should learn the KCD version used by their employer or examination. KCD-9 took effect on January 1, 2026, following its 2025 announcement by Statistics Korea. Learners using older books should verify every code, instruction, and case against the current classification.
They should also develop update discipline through coding-system release monitoring, encoder-software controls, coding competency assessment, and ICD-11 standards.
-
NHIS administers South Korea’s National Health Insurance program, while HIRA reviews healthcare benefit claims, assesses quality, and supports appropriate use of insurance resources. Providers submit claims for review, and review outcomes affect payment and may lead to correction or objection processes.
Billing professionals therefore need both insurance-program awareness and claim-review expertise, payment reconciliation, medical necessity analysis, and revenue-cycle reporting.
-
Strong Korean reading ability is highly valuable for domestic claims and Health Information Management work because candidates must interpret clinical documentation, reimbursement criteria, hospital procedures, and examination materials accurately. The necessary level extends beyond everyday conversation and includes clinical, legal, statistical, and insurance terminology.
Build a bilingual glossary using medical abbreviations, clinical documentation terms, healthcare billing acronyms, and EHR terminology. Practise complete records rather than memorizing disconnected words.
-
Remote opportunities may exist with multinational providers, RCM vendors, coding contractors, insurers, research organizations, and healthcare technology companies. Requirements depend on the destination country, employer location policy, coding system, data-security controls, language, scheduling, and employment arrangement.
For U.S.-facing work, prepare through CPT coding references, CMS-1500 billing, UB-04 claims, and commercial insurance terminology. Secure handling of patient information remains essential.