
How to Pass the CPC Certification Exam on Your First Attempt
Passing the CPC exam on your first attempt takes more than memorizing code ranges. The winning edge comes from knowing how AAPC tests judgment, how CPT guidelines hide answer clues, how ICD-10-CM details protect medical necessity, and how to move fast without becoming careless. Build your prep around real coding behavior: read documentation, identify the service, check guidelines, validate modifiers, and eliminate distractors before the clock starts punishing you.
1. Build Your CPC Exam Strategy Around How Coders Actually Work
The CPC exam rewards candidates who can think like professional outpatient coders under pressure. Your goal is to connect anatomy, procedures, diagnosis logic, modifiers, compliance, and claim impact as one workflow. Start by using AMBCI’s medical coding certification terms dictionary to lock down exam language, then pair it with the medical coding workflow terms reference so every practice question feels like a miniature chart review.
First-attempt passers usually stop studying “topics” and start studying decisions. When a question gives an operative note, you identify the body system, the approach, the exact procedure performed, the bundled services, and the documentation phrase that supports the final code. For procedure-heavy prep, rotate between the comprehensive CPT cardiology coding guide, the radiology CPT coding reference, the gastroenterology CPT code guide, and the orthopedic surgery CPT dictionary to train your eye across specialties.
The biggest trap is passive confidence. Many candidates recognize a term, choose the familiar code, and miss the detail that changed the answer: laterality, sequela, approach, separate procedure status, global period, add-on code sequencing, or payer-facing modifier logic. Use the CPT modifiers dictionary, the coding edits and modifiers guide, the medical necessity criteria guide, and the clinical documentation improvement terms dictionary until you can explain why one answer survives and the others fail.
Your study plan should protect three things: accuracy, speed, and stamina. Accuracy comes from guideline repetition. Speed comes from book navigation and elimination. Stamina comes from full-length timed blocks, because the final hour exposes weak habits. If your misses cluster around diagnosis selection, add the ICD-11 coding standards and best practices guide, the ICD-11 mental health coding dictionary, and the ICD-11 infectious diseases coding guide to strengthen diagnosis discipline.
CPC First-Attempt Pass Map: What to Master Before Exam Day
| Exam Area | What It Tests | Common First-Attempt Mistake | Best Practice Action |
|---|---|---|---|
| CPT Guidelines | Section notes, parenthetical instructions, code families, and reporting rules | Jumping to answer choices before reading the guideline that controls the code | Read the section note before selecting the final CPT code |
| ICD-10-CM Diagnosis Coding | Specificity, medical necessity, laterality, encounter type, and complication details | Choosing a broad diagnosis when the note supports a more precise one | Circle acuity, site, laterality, cause, and encounter wording in the question |
| HCPCS Level II | Supplies, drugs, DME, injections, ambulance services, and Medicare-facing items | Treating HCPCS codes as less important than CPT codes | Review common J-codes, supply codes, DME terms, and ambulance modifiers |
| Modifiers | Procedure context, payment logic, distinct services, bilateral work, and components | Adding a modifier because it sounds familiar instead of proving it from documentation | Attach every modifier to a documented reason: site, session, component, or distinct service |
| E/M Coding | Medical decision making, time, risk, data, problem complexity, and visit level | Choosing a level based on how long the note looks | Break the visit into problems, data, risk, and time before selecting the level |
| Surgery Coding | Approach, anatomical site, repair type, excision size, bundled work, and global logic | Missing bundled services inside operative reports | Underline the definitive procedure, approach, lesion size, margins, and repair method |
| Radiology | Modality, contrast, anatomical area, guidance, supervision, and component coding | Overlooking contrast wording or professional/technical component clues | Check modality, body area, contrast, guidance, and component rules together |
| Pathology and Lab | Panels, individual tests, specimens, organ/disease panels, and test combinations | Reporting individual lab tests when a panel code applies | Compare ordered tests against panel definitions before final code selection |
| Anesthesia | Base units, procedure crosswalk logic, physical status, and qualifying circumstances | Thinking like a surgery coder instead of an anesthesia coder | Identify the anesthesia service, physical status, qualifying circumstance, and procedure area |
| Medicine Section | Vaccines, injections, infusions, diagnostics, immunology, psychiatry, and specialty services | Missing administration codes or duration-based rules | Separate product, route, duration, administration, and service type |
| Cardiology | Diagnostic tests, rhythm services, catheterization, vascular access, and imaging support | Mixing diagnostic and therapeutic service families | Identify whether the service is diagnostic, interventional, monitoring, or imaging-based |
| Gastroenterology | Endoscopy extent, biopsy, lesion removal, control of bleeding, and approach | Choosing the scope family without checking how far the scope advanced | Track approach, anatomical reach, removal method, biopsy, and bundled interventions |
| Dermatology | Lesion type, lesion size, margins, excision, destruction, repair, and pathology clues | Using wound size when the rule requires lesion size plus margins | Mark benign/malignant status, lesion diameter, margins, location, and repair type |
| Orthopedics | Fracture care, manipulation, fixation, joint procedures, casting, and approach | Missing open versus closed treatment wording | Highlight treatment type, manipulation, fixation, joint/site, and follow-up context |
| Respiratory Coding | Pulmonary diagnostics, oxygen, ventilation, procedures, and diagnosis specificity | Confusing diagnosis severity with the actual procedure performed | Separate disease coding from service coding before choosing the answer |
| Neurology Coding | Nerve tests, sleep studies, neurological diagnoses, imaging, and interpretation rules | Missing body region, test type, or extremity count | Map test type, anatomical region, interpretation, and diagnosis support |
| Medical Terminology | Prefixes, suffixes, root words, procedure language, and disease terms | Guessing the body system from one familiar word fragment | Translate every term into body part, condition, and service action |
| Anatomy | Body systems, organs, locations, planes, vessels, joints, and procedure sites | Studying anatomy separately from CPT instead of tying it to codes | Review anatomy inside the CPT sections where it affects code selection |
| Compliance | Fraud risk, ethical coding, documentation standards, upcoding, and audit exposure | Treating compliance as vocabulary instead of claim-risk judgment | Connect every compliance rule to documentation proof and audit defense |
| NCCI-Style Edits | Bundling, mutually exclusive procedures, separate procedures, and modifier use | Unbundling services without a defensible documentation reason | Ask whether the note proves a distinct site, session, incision, lesion, or encounter |
| Medical Necessity | Diagnosis support, payer logic, documentation strength, and service justification | Choosing the procedure code correctly but pairing it with a weak diagnosis | Check whether the diagnosis explains why the service was reasonable and necessary |
| Claims Impact | How coding choices affect payment, denials, edits, and reimbursement flow | Thinking only about passing the exam instead of how claims behave | Review denials, EOB language, CARCs, RARCs, and payment posting logic |
| Book Navigation | Index use, tabular confirmation, section movement, symbols, and notes | Spending too long searching for codes that should be easy to locate | Practice index-to-tabular movement until code families become automatic |
| Answer Elimination | Distractor removal, code-range narrowing, and guideline conflict spotting | Trying to fully solve every answer option from scratch | Eliminate by body system, code range, modifier mismatch, and guideline conflict |
| Time Management | Question pacing, flagging strategy, stamina, and review margin | Letting one dense operative note steal time from easier questions | Use green, yellow, and red question triage during practice exams |
| Practice Exam Review | Weak-area diagnosis, speed repair, confidence tracking, and mistake patterns | Reviewing only wrong answers and ignoring lucky correct answers | Review wrong, guessed, slow-correct, and changed answers after every block |
| Final Week Prep | Guideline recall, pacing, confidence, book readiness, and fatigue control | Trying to learn too many new topics days before the exam | Consolidate notes, rehearse pacing, clean tabs, and protect sleep |
| Exam-Day Execution | Pressure control, evidence-based choices, flagging, and answer discipline | Changing answers because of panic instead of documented evidence | Trust proven clues, flag uncertain items, keep moving, and review only with a reason |
2. Master the Code Books Before You Try to Master the Questions
Your books should feel like tools, not props. Many candidates spend weeks watching lessons yet freeze because they cannot move through the index, tabular sections, symbols, guidelines, and parenthetical notes quickly. Use the CPT codes for emergency medicine guide, the complete CPT emergency medicine listing, the preventive medicine CPT coding guide, and the pediatric CPT coding reference to build section familiarity through real service categories.
Book navigation improves when you stop hunting for exact answers and start narrowing. A question about a colonoscopy with biopsy, snare removal, or control of bleeding should send you into the correct digestive endoscopy family before you inspect the final wording. A question involving infusion duration, route, drug administration, or injections should push you toward the infusion and injection therapy billing terms guide, while a diagnostic imaging question should connect to radiology billing and coding terms, lab and pathology coding essentials, and anesthesia coding and billing terms.
Annotations should be lean. Write reminders that help you decide, not paragraphs that slow you down. Mark terms like “separate procedure,” “add-on code,” “includes imaging guidance,” “do not report with,” “with contrast,” “without contrast,” “bilateral,” “unilateral,” “initial,” “subsequent,” and “sequela.” Then reinforce them with the medical abbreviations and acronyms dictionary, the health information management terms guide, the electronic health record coding terms dictionary, and the EMR documentation terms guide so chart language becomes familiar before exam day.
A strong code-book routine has three passes. The first pass teaches layout. The second pass teaches common traps. The third pass teaches speed. During each pass, ask the same questions: Which code family applies? Which guideline controls the choice? Which phrase in the documentation proves the answer? Which option violates a note? This same method works across dermatology procedures, allergy and immunology coding, dialysis coding terms, and ambulance and emergency transport coding.
3. Turn Every Practice Question Into a Missed-Revenue Investigation
The fastest way to improve is to review questions like an auditor, not a test taker. A wrong answer is rarely just “wrong.” It reveals a broken habit: skipping documentation, misreading procedure extent, ignoring modifier logic, missing diagnosis specificity, or assuming a service is separately billable. Use the medical coding audit terms dictionary, the coding ethics and standards guide, the medical coding regulatory compliance guide, and the Medicare documentation requirements guide to build audit-grade thinking.
After every practice block, sort misses into five buckets: guideline miss, terminology miss, anatomy miss, code-book navigation miss, and time-pressure miss. This is more useful than a score because it tells you what to repair tomorrow. If you consistently lose points on diagnosis-support questions, return to medical necessity criteria, SOAP notes and coding, problem lists in documentation, and the coding query process terms guide.
Treat denial language as exam training. Real claims fail when documentation, codes, modifiers, or payer rules do not line up, and CPC questions often test those same relationships. Review EOB terminology, claim adjustment reason codes, remittance advice remark codes, and claims reconciliation terms because reimbursement logic sharpens coding judgment.
Your review should include correct answers too. A correct guess can hide a dangerous weakness. Mark every question as “confident correct,” “slow correct,” “lucky correct,” “wrong but close,” or “wrong and blind.” The “slow correct” category is where first-attempt passes are often won, because saving 30–60 seconds on familiar question types creates time for complex operative reports. Build this habit with payment posting terms, medical billing reconciliation terms, healthcare claims management terms, and accurate medical billing and reimbursement.
Quick Poll: What is your biggest CPC exam prep pain right now?
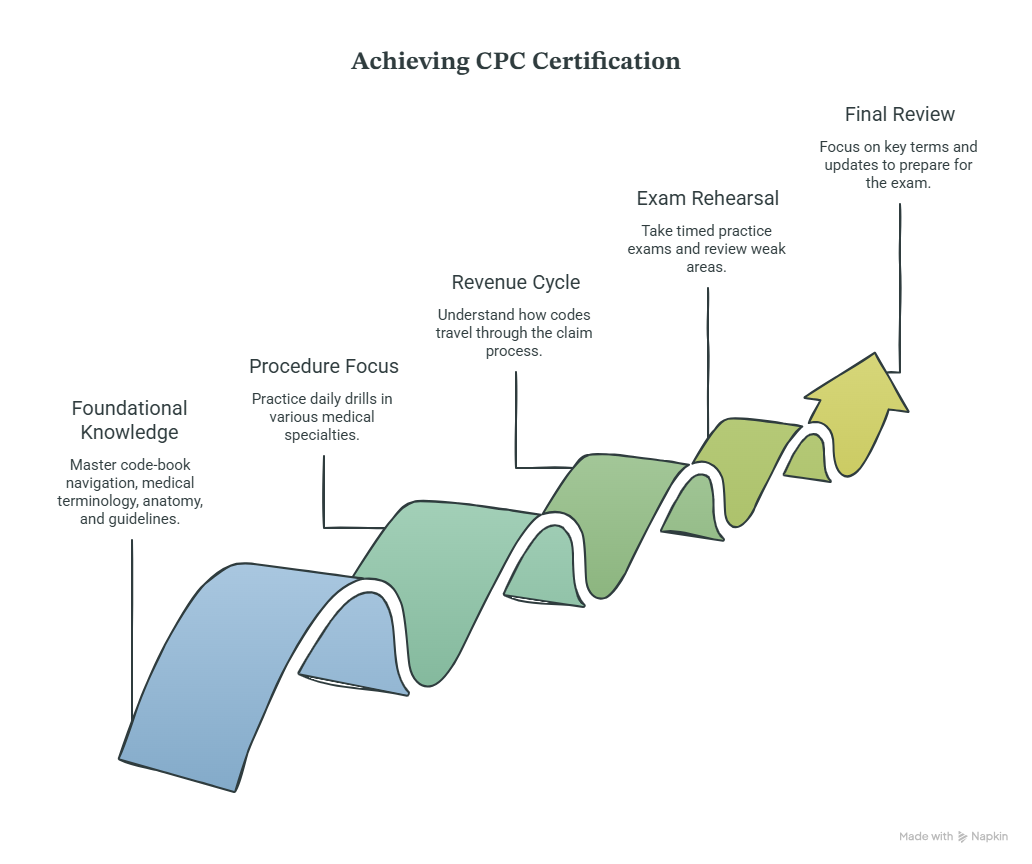
4. Use a 30-Day CPC Study Plan That Fixes Weaknesses Instead of Repeating Them
A 30-day plan works when it forces decisions, not when it repeats comfort topics. Spend the first week on code-book navigation, medical terminology, anatomy, and guideline review. Use the coding education and training dictionary, the online CPC certification program directory, the coding career development terms guide, and the coding competency and assessment terms guide to structure your foundation.
Week two should be procedure-heavy. Do short daily drills in surgery, radiology, pathology, anesthesia, medicine, and E/M, then review each miss by guideline. Add specialty refreshers from cardiology CPT coding, sleep medicine billing and coding, speech-language pathology coding, and behavioral health billing terms so less familiar chapters stop feeling like exam landmines.
Week three should combine timed practice with revenue-cycle thinking. When you choose a code, ask how that code would travel through the claim: Would the diagnosis support it? Would the modifier survive review? Would the payer deny it for bundling, missing documentation, or patient responsibility confusion? Reinforce this with revenue cycle management terms, patient responsibility and copay terms, commercial insurance billing terms, and coordination of benefits terms.
Week four should become exam rehearsal. Take full timed blocks, review flagged questions, rebuild weak areas, and reduce new learning. Study fatigue can make candidates overcorrect, change right answers, or chase rare details while ignoring common point sources. Anchor the final week with healthcare billing acronyms, medical record retention terms, encoder software terms, and coding system updates and releases to keep your review practical.
Your daily schedule should have one deep block and one repair block. The deep block covers fresh timed questions. The repair block handles misses, notes, book tabs, and guideline rereads. Keep a miss log with columns for topic, reason, correction, and next drill. This is how you convert anxiety into action. Add support from continuing education units for coders, credentialing organizations, certification renewal terms, and professional development terms so passing the exam feels connected to the job you want.
5. Control Exam-Day Pressure With a Clear Question-Handling System
Exam day should feel like execution, not discovery. Start each question by identifying what is being tested: CPT code selection, ICD-10-CM specificity, HCPCS, modifier logic, compliance, anatomy, terminology, or reimbursement reasoning. Then attack the question in the order coders use at work: service, documentation, guidelines, code family, exclusions, modifiers, diagnosis support, final answer. This method is strengthened by CMS-1500 form terms, UB-04 billing form terms, EDI billing terms, and clearinghouse terminology.
Use three pacing categories. Green questions are familiar and should move quickly. Yellow questions need guideline checking but should stay controlled. Red questions are dense operative notes or confusing modifier questions that deserve a flag and return. This prevents one brutal item from stealing time from five easier points. Practice this with charge capture terms, revenue leakage prevention, revenue cycle metrics and KPIs, and medical billing practice management systems terms, because the same triage mindset matters in real production coding.
When stuck between two answers, stop rereading everything. Identify the single difference between the options. It may be lesion size, approach, modifier, diagnosis severity, body site, bundled service, or whether the code includes a component already performed. Then return to the documentation and look only for the deciding evidence. Strengthen this habit through utilization review terms, clinical decision support terms, encounter forms and superbills, and data analytics and reporting terms.
Do not let perfection become a scoring problem. The CPC exam is passed by accumulating enough correct decisions, not by emotionally wrestling every item into certainty. Your job is to collect the points you can prove, flag the ones that need another look, and avoid panic-driven answer changes. Final readiness means you can explain your answer, find it in the book, defend it with a guideline, and move on. Keep that discipline tied to value-based care coding terms, risk adjustment coding, HCC coding definitions, and HEDIS terms because coding judgment keeps mattering after certification.
6. FAQs About Passing the CPC Certification Exam on Your First Attempt
-
Most candidates need a focused study window rather than an endless one. A realistic plan is 6–10 weeks if you already know medical terminology, anatomy, and basic coding structure; beginners may need longer because they must build both knowledge and code-book speed. Use the medical coding apprenticeship and internship terms guide, the CPC certification program directory, the CBCS certification course directory, and the CCS certification program directory to compare learning paths without turning prep into guesswork.
-
Aim for consistent scores comfortably above the passing line, but focus harder on why you miss questions than on the number itself. A candidate scoring well through guessing, slow navigation, or memorized practice sets still has exam-day risk. Track misses by CPT section, ICD-10-CM issue, modifier issue, anatomy gap, and time pressure. Support that review with coding competency assessments, claims management terms, medical billing reconciliation terms, and coding audit terms.
-
Study modifiers through documentation scenarios. A modifier should answer a specific question: Was the service distinct? Was the procedure bilateral? Was only part of the service performed? Was there a repeat service? Was a professional component reported? Was the service related to a global period? Build your drill set from the CPT modifiers dictionary, the coding edits and modifiers guide, the Medicare reimbursement reference, and the physician fee schedule terms guide.
-
Use a flag-and-return system before time pressure becomes panic. Move quickly through questions you can prove, mark dense operative notes for review, and avoid spending five minutes on a question that may be worth the same as a shorter one. Time improves when your book navigation improves, so drill index-to-code-range movement daily. Practice with CPT emergency medicine codes, radiology CPT coding, gastroenterology CPT codes, and dermatology CPT coding until section movement becomes automatic.
-
The biggest problem areas are usually modifiers, CPT guidelines, E/M logic, surgery coding, ICD-10-CM specificity, anatomy, and time management. Candidates often know definitions but fail when documentation forces a narrow choice. Fix this by studying terms inside real coding relationships. Use the medical terminology and coding workflow reference, the clinical documentation improvement dictionary, the medical necessity guide, and the surgical coding compliance terms guide.
-
Yes, because coding decisions live inside claim reality. Even when a question focuses on code selection, reimbursement logic helps you understand modifiers, medical necessity, documentation, payer edits, and denial risk. You do not need to become a billing manager before the exam, but you should understand how codes affect claims. Build that layer with RCM terms, EOB explanations, CARC definitions, and RARCs.