
Medical Billing and Coding Certification in Denmark: Complete Guide for 2026-2027
Denmark is a strong market for billing and coding learners who can connect clinical documentation, classification rules, hospital activity data, DRG logic, payer-facing evidence, and digital health workflows. A useful certification plan should strengthen medical coding workflow, revenue cycle management, clinical documentation improvement, coding audits, and Denmark-specific readiness. The real goal is simple: code cleanly, explain decisions, protect reimbursement, and prevent costly rework before claims or activity data become financial problems.
1. What Denmark-Based Learners Need to Understand First
Denmark’s healthcare system is universal, mainly tax-funded, and organized through national, regional, and municipal responsibilities, which means billing and coding work sits inside a highly structured public-health environment rather than a purely commercial insurance market. The Danish Ministry of Health describes the system as universal and built on free and equal access for citizens, while the Commonwealth Fund notes that coverage extends to legal residents and is mainly financed through general taxation. That makes accuracy in health information management, healthcare claims management, cost reporting, billing compliance, and data analytics reporting especially valuable.
For 2026-2027, a Denmark-focused learner should think in two layers. The first layer is universal coding competence: anatomy, medical terminology, diagnosis coding, procedure coding, documentation review, denial logic, claim correction, audit defense, and payment workflows. The second layer is Danish system fluency: SKS classifications, ICD-10 with national extensions, treatment classifications, DRG tariffs, activity data, hospital reporting, and region-facing reimbursement logic. AMBCI-style training can strengthen the base through medical coding certification terms, medical billing acronyms, coding education terms, coding competency assessment, and professional development.
The hardest part for beginners is usually evidence discipline. A Danish coding workflow depends on accurate clinical records, complete classification choices, defensible activity data, and correct grouping logic. If documentation is vague, the coder must recognize the gap before it becomes undercoding, overcoding, incorrect grouping, weak cost data, or avoidable follow-up work. That is why certification preparation should include medical necessity criteria, problem list documentation, SOAP note coding, EHR documentation terms, and record retention rules.
Denmark Coding Readiness Map: What to Learn Before Certification
| Skill Area | What It Means in Denmark | Why It Hits Billing or Reporting | Best Certification Prep Action |
|---|---|---|---|
| Health information management | Clinical, administrative, and activity data must remain complete and usable. | Bad data weakens reimbursement logic, planning, audits, and reporting quality. | Study documentation control, record quality, privacy, and data ownership together. |
| Coding workflow | Records move from clinical documentation to classification, grouping, and reporting. | Broken handoffs create missing diagnoses, wrong procedures, and delayed correction. | Map every step from encounter creation to final activity reporting. |
| CDI judgment | Provider documentation must support the coded condition or service. | Vague notes can distort DRG grouping, quality data, and case complexity. | Practice identifying missing acuity, causation, laterality, and treatment evidence. |
| Query process | Ambiguous records require compliant clarification before coding is finalized. | Informal corrections create inconsistency and weak audit trails. | Write clear, neutral query examples tied to exact documentation gaps. |
| Medical necessity | Services need clinical reasons that match the recorded encounter. | Unsupported services can trigger internal review, payer friction, or rework. | Link each service to indication, assessment, order, result, and plan. |
| Coding system updates | SKS and tariff resources require regular monitoring. | Outdated code choices can damage reporting, grouping, and reimbursement accuracy. | Create a quarterly update checklist and document what changed. |
| Regulatory compliance | Public healthcare financing depends on reliable records and controlled reporting. | Compliance failures affect trust, audit outcomes, and operational credibility. | Study coding rules, documentation rules, privacy rules, and audit evidence together. |
| Charge capture | Every performed service needs accurate capture in the correct workflow. | Missed services create silent leakage and distorted activity data. | Compare orders, notes, procedure logs, medication records, and coded services. |
| Revenue leakage prevention | Leaks come from missing documentation, wrong grouping, incomplete activity, or delayed correction. | Small errors accumulate into budget, reporting, and performance problems. | Track leakage by source: documentation, coding, system, workflow, or review. |
| Coding audit | Audits test whether codes match the clinical record. | Accurate codes still fail review when evidence is poorly documented. | Build workpapers showing the exact note, result, report, or provider statement used. |
| Coding edits | System checks flag conflicts, missing data, and suspicious code combinations. | Edit queues become recurring workload when root causes are ignored. | Document edit reason, correction, responsible source, and prevention step. |
| EHR documentation | Digital records drive coding, reporting, and quality review. | Template errors, missing signatures, and copied text weaken evidence. | Check author, date, clinical specificity, orders, and final assessment before coding. |
| EHR integration | Clinical, coding, registry, and finance systems must pass clean data. | Interface gaps create duplicate activity, missing services, or wrong patient context. | Learn where data enters, transforms, validates, and posts. |
| Encoder software | Tools support code selection and grouping review. | Tool dependence without judgment creates polished mistakes. | Use software output as a prompt, then validate against documentation. |
| Coding automation | Automation can suggest codes, flag gaps, and speed review. | Automated suggestions can miss secondary diagnoses or clinical nuance. | Practice human validation of automated code suggestions. |
| Data analytics | Coding quality affects hospital statistics, planning, and financial dashboards. | Poor code quality misleads leaders about case mix, utilization, and performance. | Learn basic KPI interpretation and variance investigation. |
| RCM KPIs | Leaders track productivity, accuracy, rework, denials, and correction rates. | Unmeasured coding defects keep returning. | Build a simple scorecard for accuracy, query rate, edit rate, and correction reason. |
| Surgical coding | Procedure documentation must capture anatomy, approach, device, and complications. | Missing operative detail affects procedure classification and case grouping. | Review operative notes with a structured procedure-evidence checklist. |
| Radiology coding | Imaging records need order, indication, modality, body area, and report support. | Weak indication-to-result linkage creates review friction. | Match request, clinical reason, performed study, and final report. |
| Lab and pathology coding | Laboratory data supports diagnosis, monitoring, and reporting quality. | Missing test context can weaken diagnosis support and clinical interpretation. | Connect order, specimen, result, diagnosis, and provider action. |
| Telemedicine coding | Remote encounters require clear modality, provider, patient, and service evidence. | Virtual care documentation fails when time, consent, or clinical detail is incomplete. | Create a remote-visit documentation checklist before coding. |
| Utilization review | Resource use must align with clinical need and pathway expectations. | Utilization concerns can expose missing documentation or inappropriate coding assumptions. | Review length of stay, service intensity, diagnosis support, and discharge status. |
| Reconciliation | Recorded activity, billed items, adjustments, and final outcomes must align. | Unreconciled accounts hide errors and repeat workflow defects. | Compare expected output, actual output, corrections, and final status. |
| Payment posting | Financial outcomes must be tied back to code and activity choices. | Posting errors hide underpayment, incorrect adjustment, or workflow failure. | Post with reason, source, ownership, and follow-up note. |
| Adjustment reasoning | Adjustment patterns reveal coding, documentation, or payer-rule problems. | Treating adjustments as routine creates avoidable losses. | Group adjustments into preventable, contractual, documentation, and review categories. |
| Remittance review | Payment feedback must be translated into workflow improvement. | Repeated remittance patterns show unresolved operational defects. | Create a correction log from every recurring remittance pattern. |
| Data security | Coders handle sensitive health, identity, and billing data. | Privacy mistakes damage trust, compliance, and employability. | Use minimum-access, secure-transfer, clean-desk, and controlled-storage habits. |
2. Certification Pathway: What to Study and in What Order
Start with the core language of healthcare. A Denmark-focused learner needs enough anatomy and physiology to understand diagnoses, enough medical terminology to read provider notes, enough documentation training to spot gaps, and enough billing awareness to understand why a single missing detail can change financial and reporting outcomes. Use medical abbreviations, medical coding education accreditation, CBCS exam terms, certification renewal, and CEU planning to build a structured learning base.
Next, add classification depth. The Danish Health Data Authority explains that Denmark’s classification system includes diagnoses based on WHO ICD, currently ICD-10 with national extensions, treatment classifications, and NPU terminology for laboratory medicine. The same authority notes that classification systems are updated quarterly, which makes update discipline a real workplace skill for 2026-2027 learners. Pair that local awareness with AMBCI resources on ICD coding standards, ICD cardiovascular coding, ICD oncology coding, ICD infectious disease coding, and ICD respiratory coding.
Then train on procedure logic and specialty records. Even if your Denmark role uses SKS rather than CPT, CPT-style learning still helps international coders understand how procedure definitions, documentation requirements, bundling logic, modifiers, payer edits, and specialty workflows behave. For global remote work, prioritize CPT coding references, cardiology CPT coding, emergency medicine CPT, radiology CPT coding, and CPT modifier rules. For Denmark-based hospital work, convert that same discipline into SKS, ICD-10, DRG, and documentation-quality habits.
Finally, build proof. Certification looks stronger when you can show sample case reviews, de-identified coding rationales, query drafts, denial root-cause worksheets, audit notes, and simple KPI summaries. A learner who can explain one corrected case from documentation gap to final coding decision sounds more employable than a learner who only lists course names. Build your portfolio around coding career development, coding apprenticeship terms, online exam prep resources, credentialing organizations, and coding ethics.
3. Danish Coding Systems, DRG Logic, and Documentation Skills
Denmark’s DRG environment makes classification accuracy financially meaningful. The Danish Health Data Authority states that it annually calculates DRG tariffs for somatic patients and that DRG tariffs express average hospital operating costs within each DRG group, calculated by linking actual activity and costs. Its tariff page also lists 2026 DRG tariffs and 2026 tariff guidance, so learners preparing for 2026-2027 should treat annual tariff updates as part of the job rather than a side note. Strong preparation should include physician fee schedule terms, Medicare reimbursement concepts, value-based care coding, cost reporting terms, and RCM KPI terms.
The practical skill is grouping awareness. In a DRG-linked setting, coders must understand how primary diagnosis, secondary diagnoses, procedures, complications, discharge status, age, length of stay, and clinical complexity can affect grouping and resource interpretation. The 2026 Danish tariff guidance states that patients are settled using DRG tariffs under the relevant rules and that tariffs reflect calculated direct costs of patient treatment and rehabilitation services. For learners, this means documentation review cannot be shallow. A coder needs risk adjustment thinking, HCC-style diagnosis specificity, surgical compliance, utilization review, and claims reconciliation.
The pain point is secondary diagnosis capture. Many new coders focus on the headline diagnosis and miss comorbidities that were assessed, treated, monitored, or clinically relevant. That weakens case complexity, reduces data quality, and makes records less useful for planning and analysis. A 2026 preprint trained on Danish clinical narratives from Eastern Denmark reported signs of systematic under-coding for some secondary diagnoses, which reinforces the need for careful human review even when automation helps suggest codes. Use that warning to train harder on problem list coding, clinical decision support, coding automation terms, EHR integration terms, and data security terms.
Quick Poll: What is your biggest Denmark coding readiness gap right now?
4. Career Options, Remote Work, and Employer Expectations
A Denmark-focused certification path can support roles such as medical coder, clinical coding assistant, health data coding specialist, hospital activity-data analyst, revenue cycle assistant, billing quality reviewer, documentation review specialist, claims support analyst, and coding audit coordinator. Employers value people who can read records carefully, validate codes against evidence, understand system updates, communicate with clinical teams, and explain why a coding decision is safe. Build that profile through healthcare claims management, commercial insurance billing, coordination of benefits, billing reconciliation, and denial management services.
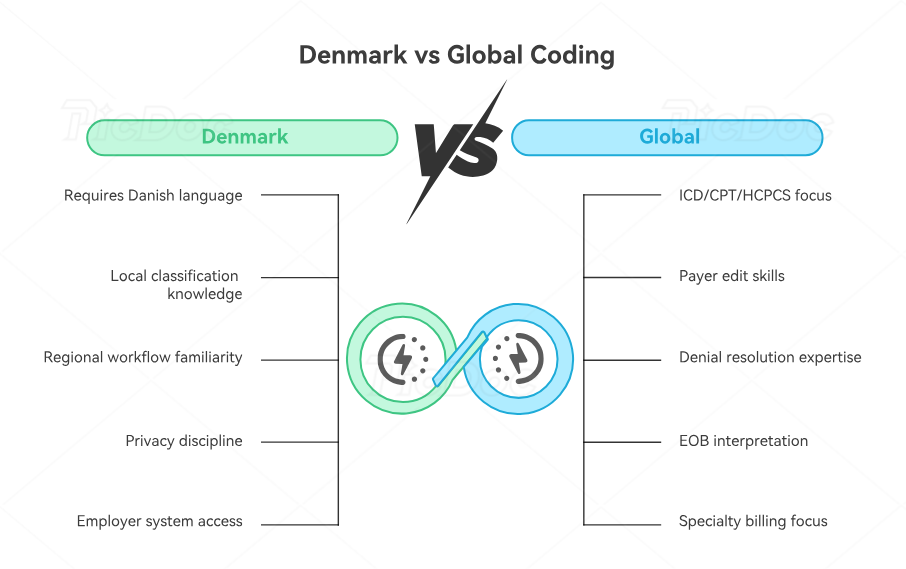
Remote work depends on the market you serve. Denmark-based remote roles may require Danish language ability, local classification knowledge, employer system access, privacy discipline, and familiarity with regional workflows. International remote roles may lean more heavily on ICD, CPT, HCPCS-style workflow, payer edits, denial resolution, EOB interpretation, and specialty billing. If you want a global profile, combine Denmark readiness with medical billing certification in the UK, medical billing certification in Australia, medical billing certification in India, medical billing certification in the Philippines, and medical billing certification in the UAE.
The strongest applicants describe problems in operational language. Instead of saying they “know coding,” they explain how they prevent missed activity, identify incomplete documentation, correct classification errors, reduce edit queues, track denial patterns, and protect reporting quality. Denmark’s health data environment rewards this mindset because clinical coding feeds much more than a bill; it supports finance, planning, quality measurement, research, and performance review. Use electronic claims submission, clearinghouse terminology, EDI billing terms, practice management systems, and RCM software terms to sound ready for real workflows.
5. Common Mistakes That Delay Hiring or Promotion
The first mistake is studying code lists without practicing record-based reasoning. Real coding work asks whether the record supports the diagnosis, whether the procedure details are complete, whether the encounter belongs in the right classification pathway, whether documentation timing is acceptable, and whether the final output can survive review. Fix this by practicing with medical necessity, encounter forms and superbills, CDI terms, coding query process terms, and medical documentation requirements.
The second mistake is ignoring Denmark’s update culture. SKS classifications, DRG tariffs, coding guidance, and system expectations can change, so a 2026-2027 learner needs version control habits. Keep a simple update log: date checked, source checked, code or tariff change, affected specialty, workflow impact, and training action. This habit makes you more useful in hospital teams because it turns regulatory change into controlled execution. Support that discipline with coding system updates, regulatory compliance, coding ethics, record storage terms, and healthcare data security.
The third mistake is staying too general. Specialty knowledge builds confidence faster because each specialty has predictable documentation traps. Cardiology needs procedure detail, device information, imaging support, and diagnosis specificity. Radiology needs indication, modality, body area, and report clarity. Infusion work needs drug, route, time, and service sequence. Behavioral health needs encounter type, risk, plan, and provider documentation. Build range with cardiology CPT, radiology billing terms, infusion billing, behavioral health billing, and allergy and immunology coding.
The fourth mistake is weak correction logic. A good coder can fix one case; a valuable coder can explain why the error happened and how to stop it from repeating. When a denial, edit, mismatch, or audit finding appears, classify it by source: documentation gap, coding choice, system mapping, eligibility issue, payer rule, tariff pathway, or posting error. Train with EOB guidance, CARC guidance, RARC guidance, payment posting, and claims reconciliation.
6. FAQs About Medical Billing and Coding Certification in Denmark
-
Yes. Certification is useful when it gives you practical coding, documentation, audit, and reporting skills that can be adapted to Danish workflows. Treat AMBCI certification as a strong foundation, then add Denmark-specific knowledge such as SKS, ICD-10 national extensions, DRG tariff logic, hospital activity reporting, privacy expectations, and employer-specific systems. Strengthen your base with medical coding certification terms, coding workflow terms, HIM terms, coding audit terms, and coding ethics.
-
Denmark-focused learners should understand SKS classifications, ICD-10 with Danish national extensions, treatment classifications, NPU terminology for laboratory medicine, and DRG tariff logic. International remote learners should also understand CPT, modifiers, claim edits, denial categories, payment posting, and remittance review. Build that mix with ICD standards, CPT coding guides, modifier guidance, coding edits, and payment posting.
-
A focused learner can build a strong foundation in a few months, then spend additional time on Danish classification, DRG, documentation, and workflow practice. Job readiness depends on language ability, case exposure, audit discipline, software comfort, and the type of employer you target. Use weekly drills: diagnosis coding, procedure review, DRG grouping logic, query writing, denial analysis, and KPI review. Support your plan with coding competency assessment, exam prep resources, CEU guidance, certification renewal, and career development.
-
Remote work is possible when your skills match the market you serve. Denmark-based remote roles may require Danish language ability, SKS and DRG familiarity, secure system access, and employer-specific training. International remote roles often require CPT, ICD, payer edits, denial management, EOB reading, and specialty billing. Build a wider profile by comparing medical billing certification in the UK, medical billing certification in Australia, medical billing certification in Saudi Arabia, medical billing certification in Qatar, and medical billing certification in Kuwait.
-
Include de-identified case reviews, diagnosis and procedure rationale, documentation query examples, DRG grouping notes, edit-resolution examples, audit worksheets, denial root-cause summaries, and simple dashboard metrics. The portfolio should prove that you can code, explain, correct, and prevent problems. Build samples using medical necessity, charge capture terms, revenue leakage prevention, audit terminology, and RCM metrics.
-
Start with core coding and billing fundamentals, then add Denmark-specific classification and DRG learning. In the first 30 days, study medical terminology, anatomy, documentation quality, diagnosis coding, procedure coding, and basic billing workflow. In the next 60 days, add SKS, ICD-10 national extensions, DRG grouping logic, audit evidence, update tracking, and specialty practice. Use medical billing certification in Pakistan, medical billing certification in Bangladesh, medical billing certification in India, medical billing certification in the Philippines, and medical billing certification in UAE to compare international pathways while building Denmark-specific readiness.