
Medical Billing and Coding Certification in Sweden: Complete Guide for 2026-2027
Sweden is a smart market for healthcare documentation, coding accuracy, clinical data quality, and international revenue cycle work. Anyone pursuing medical coding certification terms, medical billing workflow skills, revenue cycle management knowledge, coding compliance training, and medical necessity judgment from Sweden needs a clear plan. Certification helps most when it turns into real proof: accurate documentation review, defensible code selection, clean claim logic, denial reasoning, and audit-ready thinking.

1. Medical Billing and Coding Certification in Sweden: What It Actually Means in 2026-2027
Medical billing and coding certification in Sweden can support two practical career routes. One route is Sweden-facing healthcare coding, clinical documentation quality, health data reporting, and coding validation. The other route is international billing and coding support, especially for teams that expect CPT modifier knowledge, claims management terms, EOB interpretation, CARC denial analysis, and RARC remark code fluency.
For Sweden-focused work, learners should understand ICD-10-SE and KVÅ. The Swedish eHealth Agency explains that the Swedish version of ICD-10 is called ICD-10-SE and that the classification is mandatory for reporting to the National Board of Health and Welfare’s health data registers. Socialstyrelsen’s classification search service lists ICD-10-SE and KVÅ, with KVÅ divided into surgical measures and medical measures.
That matters because Sweden-facing coding and U.S.-style billing require different muscles. A Sweden-focused coder needs diagnosis coding, procedure measure coding, Swedish clinical wording, registry awareness, and documentation quality thinking. A coder targeting remote U.S. billing work needs CMS-1500 form terms, UB-04 claim logic, clearinghouse terminology, payment posting skills, and claims reconciliation habits.
Sweden also uses NordDRG in the healthcare classification and grouping environment. Socialstyrelsen describes NordDRG as containing more than 1,900 DRGs across somatic, psychiatric, outpatient, inpatient, and primary care settings. That gives Sweden-based learners another reason to understand how diagnosis, procedures, documentation, grouping, reimbursement logic, and reporting connect. Strong candidates should study coding audit terms, clinical documentation improvement terms, coding query process terms, charge capture terms, and revenue leakage prevention from the beginning.
Sweden Certification Readiness Map: What to Learn, Why It Matters, and What to Do First (25+ Rows)
| Readiness Area | What It Means in Sweden | Why It Hits Coding or Billing | Best Practice Action |
|---|---|---|---|
| Career direction | Choose Sweden-facing coding, international RCM, denial work, audit support, or documentation quality. | A blurry goal creates scattered study and weak interview answers. | Start with coding certification terms and map them to target roles. |
| ICD-10-SE awareness | Sweden-facing coding requires awareness of the Swedish ICD-10 version and its reporting purpose. | Wrong diagnosis logic weakens data quality, grouping, and clinical reporting. | Compare Swedish diagnosis logic with ICD coding standards. |
| KVÅ procedure coding | KVÅ classifies healthcare measures, including surgical and medical measures. | Procedure-measure coding affects care activity reporting, quality review, and reimbursement grouping. | Build procedure thinking through CPT modifier logic and specialty examples. |
| NordDRG awareness | Swedish reimbursement and reporting environments may involve grouping logic linked to diagnoses and procedures. | Weak grouping awareness makes documentation and code impact harder to explain. | Connect DRG thinking with cost reporting terms and RCM metrics. |
| Swedish-English terminology | Bilingual work may require moving between Swedish clinical terms and English payer or RCM language. | Terminology gaps create uncertainty in coding, appeals, and documentation review. | Build a glossary from medical abbreviations and coding references. |
| Documentation review | Every code should connect to clear clinical evidence in the record. | Unsupported codes create audit exposure and correction delays. | Train with CDI terms and SOAP note coding. |
| Medical necessity | Diagnosis, procedure, clinical indication, and payer rule must align. | Weak necessity logic causes denials, underpayment, and rework. | Use a medical necessity guide during every case drill. |
| Claim forms | Remote billing teams expect clean form logic even when the coder works outside the U.S. | Correct codes still fail when the claim field logic is wrong. | Learn CMS-1500 terms and UB-04 terms. |
| Clearinghouse edits | Claims can reject before payer adjudication due to routing, field, eligibility, or format issues. | Front-end rejections age accounts before the payer has reviewed the service. | Practice with clearinghouse terminology. |
| EOB reading | International billing roles require fast interpretation of paid, denied, adjusted, and patient-responsibility lines. | Poor EOB reading creates wrong balances and missed appeal opportunities. | Use an EOB guide until each line has a clear next action. |
| CARCs | CARCs explain claim adjustment reasons at claim or line level. | Weak CARC knowledge creates repeat denials and vague follow-up. | Keep a CARC reference beside denial drills. |
| RARCs | RARCs add payer remarks about missing information, documentation, attachments, or next steps. | Ignoring remarks wastes appeals and follow-up time. | Pair denials with the RARC dictionary. |
| Payment posting | Posting connects remittance, payer payment, contractual adjustment, and patient balance. | Posting errors distort AR, collections, and denial reports. | Study payment posting with remittance examples. |
| Patient responsibility | Patient balances depend on deductible, copay, coinsurance, coverage, and payer adjudication. | Wrong balances create disputes, collection delays, and compliance pressure. | Review patient responsibility terms. |
| COB logic | Coordination of benefits determines payer order when multiple policies exist. | Wrong payer order creates denials, refunds, and long AR loops. | Build a decision tree from COB definitions. |
| Modifier judgment | Modifiers explain distinct services, professional components, repeats, laterality, and payer exceptions. | Modifier misuse triggers edits, denials, underpayment, and audit questions. | Use the CPT modifier dictionary daily. |
| Coding edits | Edits test bundling, compatibility, frequency, payer policy, and claim logic. | Skipping edit logic creates preventable denial patterns. | Train with coding edits and modifiers. |
| Charge capture | The documented service must become the right charge before claim submission. | Missed charges create silent revenue leakage. | Audit missed revenue with charge capture terms. |
| Revenue leakage | Leakage comes from missing documentation, missed charges, weak edits, expired appeals, and poor follow-up. | Small losses across many encounters become serious monthly damage. | Use revenue leakage prevention checklists. |
| Audit defense | Every code should be defensible through documentation, coding guidance, and payer policy. | Weak evidence creates recoupment risk and team distrust. | Build habits with coding audit terms. |
| Provider queries | Queries clarify missing, incomplete, conflicting, or vague documentation. | Poor query wording creates compliance and provider relationship problems. | Practice with query process terms. |
| EHR navigation | Coders need evidence from notes, orders, reports, problem lists, results, and encounter forms. | Missing the right field leads to wrong code selection. | Review EHR coding terms and EMR documentation terms. |
| Risk adjustment | Risk coding connects documented chronic conditions to population health and payment models. | Missed conditions affect reimbursement, quality, and care planning. | Study risk adjustment coding and HCC terms. |
| Quality reporting | Some roles connect codes with outcomes, utilization, performance measures, and value-based care. | Quality knowledge helps coders grow beyond basic production work. | Connect value-based care terms with HEDIS terms. |
| Specialty exposure | Specialties have different documentation, diagnosis, procedure, modifier, and denial patterns. | General study leaves candidates weak in real production queues. | Rotate through cardiology CPT, radiology coding, and lab coding. |
| Compliance | Coders must respect documentation rules, privacy, payer policies, and ethical boundaries. | Compliance failure damages trust faster than slow productivity. | Use coding ethics and data security terms. |
| Software fluency | Remote teams expect comfort with EHRs, encoders, RCM platforms, spreadsheets, and work queues. | Slow navigation reduces productivity even when coding knowledge is strong. | Study encoder software terms and RCM software terms. |
| KPI literacy | Employers measure accuracy, clean claim rate, denial rate, AR days, productivity, and quality. | Candidates who understand metrics sound operationally ready. | Learn RCM metrics and KPIs. |
| Continuing education | Code sets, payer rules, classification updates, and documentation expectations keep changing. | Old knowledge creates fresh denial and reporting errors. | Plan renewal with CEU terms and recertification terms. |
| Career proof | A certificate creates attention; case examples prove employable judgment. | Employers trust applied examples more than generic course claims. | Build a portfolio using competency assessment terms and career development terms. |
2. Choosing the Right Certification Path From Sweden
The right certification path starts with the work you want to do. For Sweden-facing coding or clinical data roles, study ICD-10-SE, KVÅ, Swedish clinical documentation, health data reporting, and documentation quality. For international RCM roles, prioritize medical billing acronyms, commercial insurance billing terms, Medicare reimbursement basics, Medicare documentation requirements, and accurate billing and reimbursement.
A strong certification program should train four layers. The first layer is coding: diagnoses, procedures, modifiers, laterality, acuity, complications, and documentation support. The second layer is claim construction: eligibility, payer rules, authorizations, claim fields, attachments, and edits. The third layer is adjudication: EOB interpretation, CARC adjustment codes, RARC remark codes, payment posting, and billing reconciliation. The fourth layer is audit defense: every code must point to evidence.
Sweden-based learners should avoid a common trap: collecting certification language while staying weak in production decisions. A strong candidate can explain why a diagnosis supports a service, why a modifier is necessary, why a claim rejected, how a remittance moved the balance, and what evidence would survive audit. That requires coding audit vocabulary, coding ethics standards, HIM terms, utilization review terms, and claims management discipline.
Language positioning also matters. Swedish helps with local documentation, ICD-10-SE context, KVÅ terminology, provider communication, and registry-facing roles. English helps with global RCM, U.S. payer rules, medical policies, appeal writing, and remote billing operations. A candidate who can combine both with EHR integration terms, practice management system terms, encoder software terms, medical abbreviations, and data analytics reporting terms can build a stronger, more flexible career story.
3. Skills Sweden-Based Coders Must Prove Before Employers Trust Them
Employers trust coders who can follow the full encounter-to-payment chain. That means reading the record, identifying the billable service, validating the diagnosis, applying procedure logic, recognizing missing documentation, fixing edits, and explaining the result. Sweden-based learners should build that ability through SOAP note coding, problem list documentation, medical record retention terms, clinical decision support terms, and EMR documentation terms.
Diagnosis accuracy is the first proof area. Beginners often grab the visible diagnosis and miss acuity, cause, laterality, status, complication, episode context, or chronic condition evidence. That weakens medical necessity, risk capture, reporting quality, and claim strength. Train your eye with ICD-11 mental health definitions, neurological disorder codes, respiratory disease coding, cardiovascular code references, and oncology coding references.
Procedure logic is the second proof area. A coder can understand diagnosis coding and still struggle when procedures, documentation thresholds, components, modifiers, and edits enter the queue. Specialty reps create practical confidence. Rotate through emergency medicine CPT codes, radiology CPT references, orthopedic surgery CPT coding, dermatology CPT coding, and infusion billing terms.
Denial thinking is the third proof area. A serious coder can explain why a claim failed, what evidence is missing, who owns the fix, and which correction has the highest payment chance. That skill grows from working with coordination of benefits definitions, claim adjustment reason code directories, RARC explanations, workers compensation billing resources, and collections and bad debt terms. Denials reveal process weakness; trained coders know how to read that signal.
Quick Poll: What is your biggest certification blocker in Sweden right now?
4. A Practical 12-Week Study Plan for Certification Success in Sweden
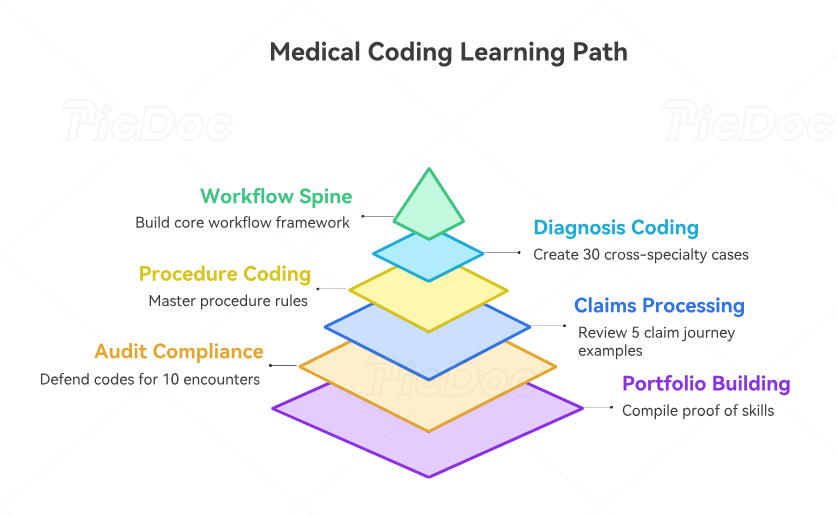
Weeks 1 and 2 should build the workflow spine. Learn how an encounter becomes documentation, how documentation becomes diagnosis and procedure codes, how codes become charges, how charges become claims, and how claims become payment, denial, adjustment, or patient responsibility. Read medical coding workflow terms, charge capture terms, RCM terminology, healthcare claims management, and billing reconciliation terms. This mental map makes later study easier because every topic has a revenue cycle location.
Weeks 3 and 4 should focus on diagnosis coding, clinical specificity, and documentation support. Create 30 short cases across primary care, cardiology, respiratory care, neurology, oncology, infectious disease, behavioral health, and post-acute care. For each case, write the diagnosis evidence, missing documentation, code rationale, and medical necessity connection. Use behavioral health billing terms, cardiovascular disease code references, infectious disease coding, oncology references, and medical necessity criteria.
Weeks 5 and 6 should focus on procedure coding, modifiers, specialty patterns, and documentation thresholds. Build a working table with common services, required note elements, possible modifiers, bundling issues, payer edit risks, and appeal evidence. Rotate through cardiology CPT procedures, gastroenterology CPT codes, pediatric CPT references, preventive medicine coding, and anesthesia billing terms.
Weeks 7 and 8 should move into claims and remittance. Take five claim examples and explain each journey from encounter to final balance. Include eligibility, claim form fields, clearinghouse checks, payer edits, denial reasons, payment posting, patient responsibility, and appeal options. Use clearinghouse terminology, EDI billing terms, EOB interpretation, payment posting guidance, and patient responsibility definitions.
Weeks 9 and 10 should sharpen audit, compliance, CDI, and query judgment. Select ten encounters and write a defense for each code. Then write a compliant query for unclear, conflicting, incomplete, or vague documentation. The question to train is simple: “What does the record prove?” Use coding ethics standards, CDI terminology, query process terms, surgical coding compliance, and Stark Law and Anti-Kickback terms.
Weeks 11 and 12 should turn knowledge into proof. Build a small portfolio with de-identified sample cases, denial explanations, modifier examples, query examples, and a one-page revenue cycle map. Add a resume section showing certification progress, ICD-10-SE and KVÅ awareness, claim workflow knowledge, specialty exposure, bilingual terminology strength, and audit readiness. Strengthen your wording with career development terms, coding education terms, credentialing organization terms, apprenticeship and internship terms, and professional development terms.
5. Career Opportunities After Medical Billing and Coding Certification in Sweden
Certification can support several career lanes from Sweden. International RCM companies may need coders, billing assistants, denial analysts, payment posters, charge entry staff, audit support workers, quality reviewers, and specialty coding trainees. Strong applications connect training to operational value: cleaner claims, fewer denials, faster correction, stronger documentation, safer audits, and better revenue visibility. Use RCM KPI terms, claims reconciliation terms, denial management resources, billing software terms, and electronic claims submission platforms.
Sweden-facing health information roles can involve clinical coding support, documentation quality, hospital statistics, health data reporting, registry quality, audit preparation, or administrative billing workflows. Socialstyrelsen describes the National Patient Register as a basis for statistics on diseases and treatments in Swedish specialised care, which shows why accurate coding and documentation have value beyond one claim or one invoice. Strengthen this path with HIM terms, data security terms, medical record storage terms, data analytics terms, and cost reporting terms.
Remote work can be attractive, yet it rewards proof over hope. Many beginners fail interviews because their resume says “certified” while their answers reveal weak claim logic, denial reasoning, modifier confidence, and audit evidence. Prepare three stories before applying: one code selection story, one denial correction story, and one documentation query story. Each story should mention the record, the coding decision, the payer issue, the correction, and the revenue result. Use coding competency assessment terms, medical coding automation terms, RCM software terms, practice management systems, and EHR integration terms.
Specialization is the fastest way to sound serious. Pick one area after building the base, then study documentation patterns, CPT families, common modifiers, medical necessity rules, denial causes, and appeal evidence. Good specialty lanes include telemedicine coding, radiology coding, lab and pathology coding, sleep medicine billing, hospice and palliative care coding, and speech-language pathology coding. Depth creates sharper interviews, stronger accuracy, and better long-term growth.
6. FAQs About Medical Billing and Coding Certification in Sweden
-
Yes. Certification is useful when it is connected to practical documentation, coding, claims, denial, and audit skills. Sweden-based learners can use certification for international RCM roles, remote billing support, documentation quality work, health information pathways, and specialty coding preparation. Build your foundation with medical coding certification terms, RCM terms, accurate reimbursement guidance, coding compliance, and coding career terms.
-
Start with your target market. For Sweden-facing work, learn ICD-10-SE, KVÅ, Swedish documentation language, and NordDRG awareness. For U.S.-style remote billing, learn ICD-10-CM concepts, CPT, HCPCS, modifiers, claim forms, EOBs, CARCs, and RARCs. A practical plan should include ICD coding standards, CPT modifier usage, claim adjustment codes, RARC definitions, and EOB reading.
-
Remote work is possible when your certification is backed by proof of applied skill. Employers want coders who understand documentation, code selection, claim forms, payer edits, denial correction, payment posting, and audit evidence. Build a portfolio using SOAP note coding, CMS-1500 terms, clearinghouse terminology, payment posting, and claims reconciliation.
-
A focused beginner can build a strong foundation in about 12 weeks, then continue with specialty practice, mock cases, and real-world claim scenarios. The timeline depends on healthcare background, English fluency, Swedish clinical vocabulary, and weekly study hours. A strong schedule covers medical billing workflow, medical necessity, coding edits, coding audits, and competency assessment.
-
The biggest mistake is studying code lists without studying the documentation and billing chain. Real work requires documentation review, diagnosis support, procedure logic, medical necessity, claim form accuracy, payer edits, remittance reading, denial correction, and audit defense. Beginners should study charge capture, revenue leakage prevention, denial management, patient responsibility, and coordination of benefits together.
-
Swedish helps with Sweden-facing clinical documentation, ICD-10-SE context, KVÅ language, provider communication, and health information work. English helps with U.S.-style billing, payer policies, global RCM platforms, medical policies, EOBs, and appeal writing. Candidates with both languages can stand out by combining medical abbreviations, EMR documentation terms, EHR coding terms, HIM terminology, and healthcare data security.