
Medical Billing and Coding Certification in Germany: Complete Guide for 2026-2027
Germany is a serious market for healthcare documentation, reimbursement accuracy, and global revenue cycle work. Anyone pursuing medical coding certification terms, medical billing workflow skills, revenue cycle management knowledge, and coding compliance training from Germany needs a practical plan, because employers care about proof, accuracy, speed, audit confidence, and clean claim logic. This guide breaks down the certification path, the billing systems to understand, the skills to build, and the mistakes that quietly block beginners from paid coding roles.
1. Medical Billing and Coding Certification in Germany: What It Actually Means in 2026-2027
Medical billing and coding certification in Germany usually means building a career-ready skill set for international coding, U.S.-style claims work, healthcare documentation review, payer communication, and revenue cycle operations. The strongest candidates understand ICD coding foundations, CPT procedure coding, claim adjustment reason codes, remittance advice remark codes, and medical necessity criteria before they chase job applications.
Germany has its own healthcare coding environment. ICD-10-GM is the official diagnosis classification used in inpatient and outpatient medical care, and BfArM lists ICD-10-GM 2026 as the currently valid version. OPS is the official classification for operations, procedures, and general medical measures. ICD-10-GM and OPS form the basis for German reimbursement systems in outpatient and inpatient care, so Germany-based learners should understand how local code logic differs from U.S.-style ICD-10-CM, CPT, and HCPCS workflows.
That difference matters for career planning. A learner targeting German hospitals, coding quality, or documentation review needs ICD-10-GM and OPS awareness. A learner targeting remote billing teams, U.S. practices, clearinghouses, or offshore RCM work needs strong command of CMS-1500 billing terms, UB-04 claim logic, payment posting, claims reconciliation, and denial management basics. The best certification route is the one that proves you can move from documentation to codes, from codes to claims, from claims to remittance, and from remittance to corrected revenue.
Germany Certification Readiness Map: What to Learn, Why It Pays, and What to Do First (25+ Rows)
| Readiness Area | What It Means in Germany | Why It Hits Billing | Best Practice Action |
|---|---|---|---|
| Certification goal | Decide whether you want local coding quality work, global RCM work, or U.S.-style claims support. | A vague goal creates scattered studying and weak interview answers. | Start with coding certification terms and map them to real roles. |
| Diagnosis coding | Germany uses ICD-10-GM locally, while international RCM roles may use ICD-10-CM or ICD-11 references. | Wrong diagnosis specificity creates medical necessity gaps and denial risk. | Study ICD coding standards with payer-facing examples. |
| Procedure coding | Local German work may involve OPS, while U.S.-focused billing requires CPT and HCPCS logic. | Procedure mismatch can destroy reimbursement even when the diagnosis is correct. | Build CPT strength through modifier usage and specialty examples. |
| Medical necessity | A code must support the service, the record, and the payer policy. | Necessity failures trigger denials, takebacks, audits, and provider frustration. | Use a medical necessity checklist before claim release. |
| Claim forms | Global billing teams expect clean claim form knowledge even when coders work remotely. | A good code in the wrong field still becomes a bad claim. | Learn CMS-1500 terms and UB-04 billing fields. |
| EOB reading | German learners targeting U.S. billing roles must read payer payment explanations fluently. | Teams lose revenue when staff read paid, denied, adjusted, and patient responsibility lines poorly. | Practice with an EOB guide until each line tells a story. |
| CARCs | CARCs explain claim-level and line-level adjustment reasons. | Weak CARC knowledge creates lazy rework and repeat denials. | Use the CARC reference during every denial drill. |
| RARCs | RARCs add remark detail that explains what the payer expects next. | Ignoring remarks leads to pointless resubmissions and aging AR. | Pair each denial with the RARC dictionary. |
| Charge capture | The charge must exist, match the service, and flow correctly into billing. | Missed charges create silent revenue leakage that reports rarely expose fast enough. | Use charge capture terms to audit front-end loss. |
| Revenue leakage | Leakage happens when documentation, codes, charges, claims, or follow-up fail. | Small misses across many encounters become large monthly losses. | Study revenue leakage prevention with examples. |
| Audit readiness | Certification should train you to defend code selection with documentation evidence. | Unsupported codes can trigger recoupments and credibility loss. | Build evidence habits with coding audit terms. |
| CDI awareness | Clinical documentation improvement connects provider language to coding precision. | Vague notes force downcoding, queries, delays, and avoidable rework. | Use CDI terms to improve query judgment. |
| Provider queries | Coders must know when the record needs clarification. | Bad queries create compliance risk and weak provider relationships. | Practice compliant wording with query process terms. |
| EHR documentation | Most coding evidence lives inside structured and unstructured EHR fields. | Missing the right note section leads to undercoding or overcoding. | Review EHR coding terms and EMR documentation terms. |
| Clearinghouse workflow | Clearinghouses catch many formatting and payer-routing errors before payer adjudication. | Front-end rejections age accounts before the payer even reviews the claim. | Learn clearinghouse terminology early. |
| Payment posting | Payment posting connects remittance data to patient balances and payer follow-up. | Posting errors distort AR reports, collections, and appeal timing. | Study payment posting with real scenarios. |
| Patient responsibility | Patient balance rules affect copays, coinsurance, deductibles, and collections. | Poor balance handling causes patient disputes and compliance headaches. | Use patient responsibility terms during EOB review. |
| Coordination of benefits | COB decides payer order when more than one policy exists. | Wrong payer order can create denials, refunds, and long AR loops. | Build a COB decision tree from COB definitions. |
| Modifiers | Modifiers explain service circumstances, bundling exceptions, laterality, repeat services, and professional or technical components. | Modifier mistakes are among the fastest ways to create payer edits. | Use the CPT modifier dictionary daily. |
| Coding edits | Edits check bundling, incompatibility, frequency, payer rules, and documentation logic. | Ignoring edits creates preventable denials and messy appeals. | Train with coding edits and modifiers. |
| Risk adjustment | Risk coding links documented conditions to population risk and payment models. | Missed chronic conditions affect reimbursement, quality reporting, and care planning. | Study risk adjustment coding and HCC definitions. |
| Quality reporting | Some roles expect understanding of quality measures and value-based payment signals. | Weak quality knowledge limits growth beyond entry-level coding. | Connect value-based care terms with HEDIS terms. |
| Specialty coding | Specialties expose different CPT, modifier, diagnosis, and documentation patterns. | Generic study leaves candidates weak in real production queues. | Rotate through cardiology CPT, radiology CPT, and lab coding. |
| Compliance | A certified coder must understand documentation support, privacy, payer rules, and ethical boundaries. | Compliance errors damage trust faster than speed errors. | Use coding ethics and data security terms. |
| Software fluency | Remote teams expect comfort with EHRs, encoders, RCM platforms, spreadsheets, and work queues. | Slow navigation reduces productivity even when coding knowledge is good. | Review encoder software terms and RCM software terms. |
| KPI literacy | Billing teams measure accuracy, denial rate, days in AR, clean claim rate, and productivity. | Candidates who cannot discuss metrics struggle to sound job-ready. | Learn RCM metrics and KPIs. |
| Continuing education | Coding rules, payer edits, and reimbursement guidance keep changing. | Old knowledge creates fresh denials. | Plan renewal with CEU terms and recertification terms. |
| Career proof | A certificate gets attention, while case examples prove applied skill. | Employers want evidence that you can handle messy documentation and payer responses. | Build a portfolio using career development terms and competency assessment terms. |
| Job application positioning | Germany-based applicants should explain time zone coverage, language ability, system familiarity, and claims knowledge. | A generic resume makes international experience look unfocused. | Use professional development terms to sharpen your profile. |
2. Choosing the Right Certification Path From Germany
The right path starts with your target employer. If you want global RCM support, prioritize medical billing acronyms, accurate medical billing and reimbursement, commercial insurance billing terms, Medicare reimbursement basics, and Medicare documentation requirements. If you want German healthcare documentation quality work, add ICD-10-GM, OPS, German clinical terminology, and payer documentation expectations to your plan.
A strong certification program should teach four layers. The first layer is code selection: diagnosis, procedure, modifiers, bundling, laterality, frequency, and documentation support. The second layer is claim construction: forms, clearinghouse edits, payer policies, authorizations, and attachments. The third layer is adjudication: EOB interpretation, CARC denial reasons, RARC remarks, payment posting, and billing reconciliation. The fourth layer is audit defense: every code must point back to the chart.
Germany-based learners should avoid the common “memorize code sets first” trap. Coding careers reward judgment, and judgment comes from messy cases. A good study week includes a documentation review case, a claim form drill, a denial analysis, a modifier scenario, and a compliance checkpoint. That combination prepares you for coding audit terminology, coding ethics, HIM terminology, utilization review concepts, and claims management terms in one practical workflow.
Your certification choice should also match your language and market plan. English fluency matters for U.S.-style coding, payer policies, EOBs, appeal letters, and remote team communication. German fluency matters for local records, ICD-10-GM context, OPS terminology, and provider communication. Candidates who can work across both languages have a strong story, especially when they combine EHR integration terms, practice management system terms, encoder software terms, medical abbreviations, and data analytics reporting terms.
3. Skills Germany-Based Coders Must Prove Before Employers Trust Them
Employers care about production behavior. They want coders who can read the note, identify the billable service, validate the diagnosis, apply the right procedure logic, detect missing documentation, route a query, fix an edit, and explain the result. That is why your study plan should move through SOAP note coding, problem list documentation, medical record retention terms, clinical decision support terms, and EMR documentation vocabulary.
The first proof area is diagnosis accuracy. Beginners often select the most visible condition in the chart and miss causality, acuity, status, complications, and encounter context. That leads to weak medical necessity and poor risk capture. Build drills around ICD-11 mental health definitions, neurological disorder coding, respiratory disease coding, cardiovascular code references, and oncology coding references so your eye learns specificity.
The second proof area is procedure and specialty logic. A coder who understands general concepts still needs specialty reps, because a dermatology biopsy, an ED visit, an infusion encounter, a radiology read, and an orthopedic repair create different documentation risks. Rotate through emergency medicine CPT codes, radiology billing and coding terms, orthopedic surgery CPT coding, dermatology CPT coding, and infusion billing terms.
The third proof area is denial thinking. A coder should be able to explain why a claim failed, what evidence is missing, which party owns the fix, and which correction has the highest chance of payment. That requires COB definitions, claim adjustment code knowledge, appeal-ready remittance terms, workers compensation billing resources, and collections and bad debt terms. This is where beginners become valuable: they stop treating denials as chores and start treating them as evidence.
Quick Poll: What is your biggest certification blocker in Germany right now?
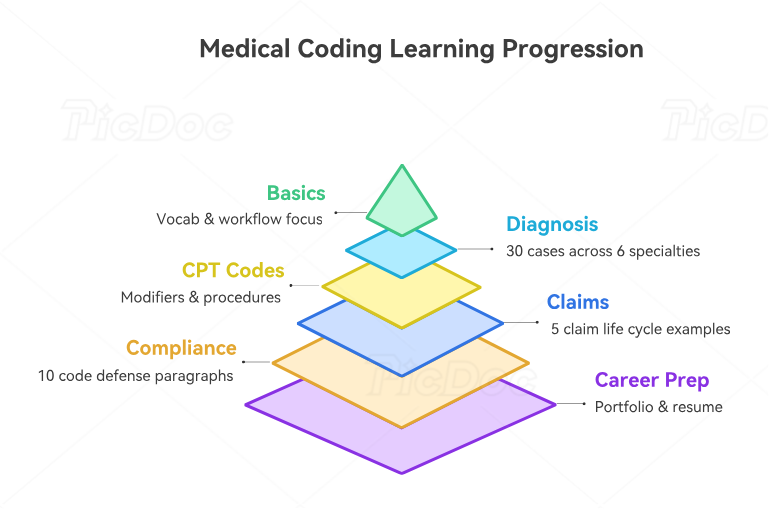
4. A Practical 12-Week Study Plan for Certification Success in Germany
Weeks 1 and 2 should focus on vocabulary and workflow. Learn how a patient encounter becomes documentation, how documentation becomes codes, how codes become charges, how charges become claims, and how claims become payment or denial. Your daily reading should include medical coding workflow terms, charge capture terms, RCM terminology, healthcare claims management, and billing reconciliation terms.
Weeks 3 and 4 should focus on diagnosis coding and documentation support. Build 30 short cases across primary care, cardiology, respiratory care, neurology, oncology, and behavioral health. For each case, write the diagnosis evidence, missing documentation, code rationale, and medical necessity connection. Use behavioral health billing terms, cardiovascular disease code references, infectious disease coding, oncology references, and medical necessity criteria.
Weeks 5 and 6 should focus on CPT, modifiers, and procedure patterns. Build a table of common services, required documentation, possible modifiers, bundling issues, and payer edit risks. Move through cardiology procedure CPT, gastroenterology CPT codes, pediatric CPT references, preventive medicine CPT coding, and anesthesia billing terms.
Weeks 7 and 8 should focus on claims and remittance. Take five claim examples and force yourself to explain the life of each claim from encounter to final balance. Include payer edits, clearinghouse checks, denial reasons, payment posting, patient responsibility, and appeal options. The best resources here are clearinghouse terminology, EDI billing terms, EOB interpretation, payment posting guidance, and patient responsibility definitions.
Weeks 9 and 10 should focus on audit, compliance, CDI, and query discipline. Take ten sample encounters and write a one-paragraph defense for each code choice. Then write a query when the documentation is unclear. This builds the exact skill employers need when claims are challenged. Use coding ethics standards, CDI terminology, query process terms, surgical coding compliance, and Stark Law and Anti-Kickback terms.
Weeks 11 and 12 should turn studying into career evidence. Build a small portfolio with de-identified sample cases, denial explanations, modifier examples, and a one-page workflow map. Add a resume section showing certification progress, specialty exposure, claim workflow knowledge, and audit readiness. Strengthen your wording with career development terms, coding education terms, credentialing organization terms, apprenticeship and internship terms, and professional development terms.
5. Career Opportunities After Medical Billing and Coding Certification in Germany
Germany-based candidates can position themselves for several kinds of work. International RCM companies may need coders, billing assistants, denial analysts, payment posters, audit support staff, credentialing support, quality reviewers, and specialty coding trainees. The strongest applications connect certification to specific operational value: cleaner claims, fewer denials, faster follow-up, stronger documentation, safer audits, and clearer provider queries. Use RCM KPI terms, claims reconciliation terms, denial management resources, billing software terms, and electronic claims submission platforms to speak in employer language.
Local healthcare-adjacent opportunities can involve documentation quality, hospital reimbursement support, coding validation, analytics, audit preparation, or administrative billing support. For these routes, Germany-specific code systems, German medical language, privacy expectations, and hospital process awareness become powerful additions. Candidates should understand the relationship between diagnoses, procedures, reimbursement groups, quality reporting, and documentation evidence. Strengthen this side with HIM terms, data security terms, medical record storage terms, data analytics terms, and cost reporting terms.
Remote work is attractive, yet the hiring bar is unforgiving. Entry-level candidates often fail because their resume says “certified” while their interview answers show no claim workflow, no denial reasoning, no modifier confidence, and no audit trail discipline. Fix that before applying. Prepare three stories: one code selection story, one denial correction story, and one documentation query story. Each story should mention the record, the code, the payer issue, the correction, and the revenue impact. Use coding competency assessment terms, medical coding automation terms, RCM software terms, practice management systems, and EHR integration terms to sharpen those stories.
The long-term advantage is specialization. A Germany-based coder who learns one specialty deeply can stand out faster than a generalist. Choose a lane based on demand and personal fit: telemedicine coding, radiology coding, lab and pathology coding, sleep medicine billing, hospice and palliative care coding, or speech-language pathology coding. Depth creates confidence, and confidence shows up in interviews.
6. FAQs About Medical Billing and Coding Certification in Germany
-
Yes. Certification is useful when it is paired with practical coding, documentation, claims, and denial skills. Germany-based learners can use certification for international billing teams, remote RCM support, documentation quality roles, and healthcare administration pathways. Build your base with medical coding certification terms, RCM terms, accurate reimbursement guidance, coding compliance, and coding career terms.
-
Start with your target market. For U.S.-style jobs, learn ICD-10-CM concepts, CPT, HCPCS, modifiers, claim forms, EOBs, CARCs, and RARCs. For Germany-facing work, learn ICD-10-GM and OPS awareness alongside German documentation language. A practical plan should include ICD coding standards, CPT modifier usage, claim adjustment codes, RARC definitions, and EOB reading.
-
Remote work is possible when your certificate is backed by demonstrable skill. Employers want coders who understand documentation, codes, claim forms, payer edits, denials, appeals, and audit evidence. Build a small proof portfolio using SOAP note coding, CMS-1500 terms, clearinghouse terminology, payment posting, and claims reconciliation.
-
A focused beginner can build a strong foundation in about 12 weeks, then continue with specialty practice and mock cases. The timeline depends on English fluency, German medical vocabulary, healthcare background, and weekly study hours. A useful schedule covers medical billing workflow, medical necessity, coding edits, coding audits, and competency assessment.
-
The biggest mistake is studying code lists in isolation. Real billing work requires a complete chain: documentation, code selection, medical necessity, claim fields, payer edits, remittance, correction, and audit defense. Beginners should study charge capture, revenue leakage prevention, denial management, patient responsibility, and coordination of benefits together.
-
German language skills help for local documentation, ICD-10-GM context, German provider communication, and healthcare administration in Germany. English skills help for international RCM teams, U.S. payer policies, EOBs, appeal language, and remote billing workflows. Candidates with both can build a stronger profile by combining medical abbreviations, EMR documentation terms, EHR coding terms, HIM terminology, and healthcare data security.